Introduction
More and more, Chiropractors are becoming interested in rehabilitation of the abnormal cervical lordosis due to its potential relationship with a number of patient health disorders.1-3 Chiropractic techniques often recommend the use of both in office equipment as well as supplementation of at home orthotics for rehabilitation of the abnormal cervical lordosis in appropriate cases,4 while other chiropractors use at home orthotics as the primary means of the rehabilitation of the cervical lordosis. There are a number of home devices to choose from and not enough information on when it is and is not appropriate to use these devices for a given patient presentation.
In the present article, I would like to discuss the appropriate use of two common corrective cervical orthotic devices aimed at rehabilitation of abnormal cervical curvatures by presenting appropriate indications and contra-indications for the use of these devices.
Non-Compression 3-Point Bending
Cervical orthotics provoke a passive 3-point bending force that is generally well tolerated by most patients, as it does not apply compression to the cervical column during patient application. Patient size and the specific abnormality of the cervical lordosis influence the size and choice of what type of cervical orthotic is appropriate for a specific patient. For example, the amount of anterior or posterior head translation dictates the size of the cervical orthotic to be used, however the shape in the cervical lordosis determines the location of the peak of the device (C6-T1, C4-C6, or C2-C4).
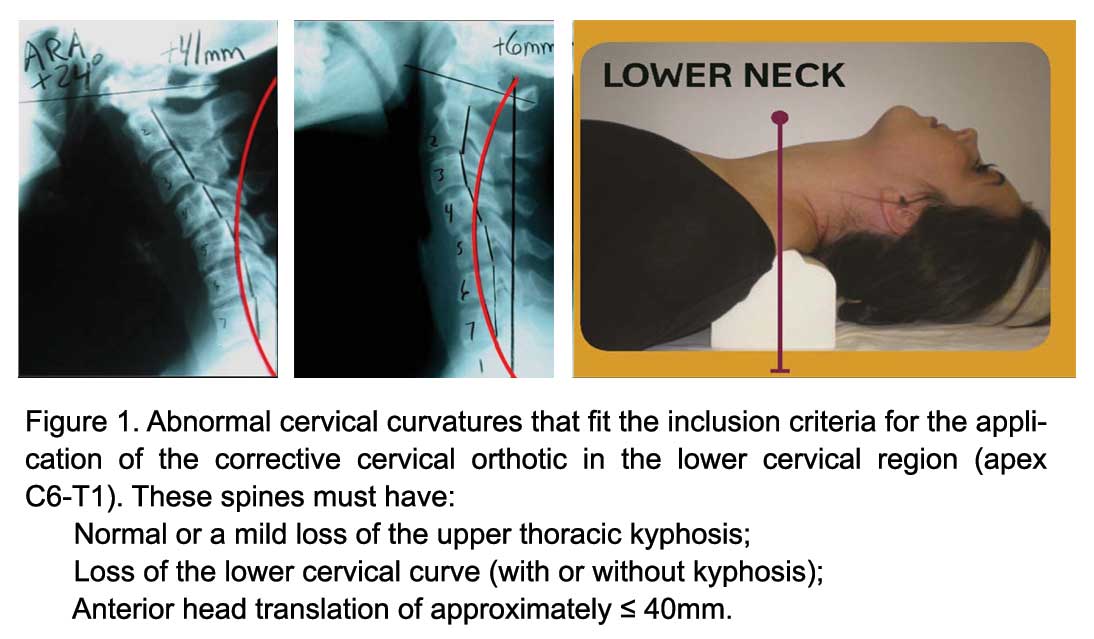
There are three primary placements of this cervical orthotic, but only the lower cervical/upper thoracic placement will be discussed. Figure 1
Indications for the Cervical Orthotic Lower Neck Placement:
Upper thoracic/lower cervical placement. This placement of the orthotic will cause significant posterior head translation unless the large device is used. A lower cervical placement will increase the upper thoracic curve and increase the overall cervical lordosis. Specifically, this placement should be used for straightened or kyphotic lower cervical segments with loss of upper thoracic kyphosis and anterior head translation of approximately ≤ 40mm. (Figure 1)
Contra-indications for the Cervical Orthotic:
Quite simply put, the contra-indications for this cervical remodeling orthotic device would be the opposite of the indications listed above and many are the indications for the compression-extension wedge below.
Compression-Extension Remodeling Wedge 
The compression extension cervical orthotic device is a common tool available in the chiropractic profession today with several brands on the market. (Figure 2) The device creates the combination of posterior head translation, cervical extension, and compression force down the long-axis of the spine. Patients must be screened for tolerance to this position and loading; canal stenosis would be contra-indicated for this device.
Problematically, the compression extension wedge also creates an anterior translation of the thoracic spine and an extension of the mid-upper thoracic kyphosis. Typically speaking, the wedge only comes in one size (adult) and, thus, patient selection must be considered when using these devices; pediatric cases don’t fit well on this.
Indications for the Compression-Extension Wedge:
The compression-extension wedge will correct-reduce anterior head translation with loss of the cervical lordosis. The patient’s posterior vertebral body margins (black dashed-line) must be well anterior of the ideal cervical lordosis (red-line after Harrison et al.2). Head translation forward ≥ 25mm and up to ≈ 70 mm typically responds well to this device. However, the patient must also have posterior thoracic translation and increased mid- and upper-thoracic kyphosis, as the wedge will cause an opposite effect. Figure 2
 Contra-indications for the Compression-Extension Wedge:
Contra-indications for the Compression-Extension Wedge:
Quite simply put, the Contra-Indications for these cervical remodeling orthotic devices would be the opposite of the indications for those listed above and many are the indications for the non compression three-point-bending devices.
SUMMARY
All home cervical corrective orthotic devices, such as the two shown herein, have indications and contra-indications for appropriate patient application. The cervical corrective orthotic should be fit to the following patient presenting conditions: 1) their symptomatology and severity of spinal arthritis/disc disease, 2) their ability to perform specific movements, 3) their presenting posture of the head and thoracic region, 4) their configuration of the cervical curvature, 5) the presence of any unstable segments, and 6) their configuration of the mid-upper thoracic kyphosis. I hope this presentation assists in your delivery of effective at home devices for rehabilitation of the abnormal cervical lordosis.
Dr. Deed will be presenting a comprehensive, contemporary review of this topic at the upcoming 32nd CBP Annual Conference on Sept. 24-26th, in Scottsdale, AZ.
Deed E. Harrison, D.C. is President CBP Seminars, Inc., Vice President CBP® Non-Profit, Inc., Chair PCCRP Guidelines, Editor—AJCC.
References
1.Harrison DE, Betz J, Ferrantelli JF. Sagittal spinal curves and health. JVSR 2009 July 31, pp 1-8.
2.Harrison DD, Harrison DE, Janik TJ, Cailliet R, Haas JW, Ferrantelli J, Holland B. Modeling of the Sagittal Cervical Spine as a Method to Discriminate Hypo-Lordosis: Results of Elliptical and Circular Modeling in 72 Asymptomatic Subjects, 52 Acute Neck Pain Subjects, and 70 Chronic Neck Pain Subjects. Spine 2004; 29:2485-2492.
3.McAviney J, Schulz D, Richard Bock R, Harrison DE, Holland B. Determining a clinical normal value for cervical lordosis. J Manipulative Physiol Ther 2005;28:187-193.
4.Harrison DE, Harrison DD, Haas JW. CBP Structural Rehabilitation of the Cervical Spine. Chapters 2 & 6. CBP Seminars, 2002; pgs:147-151. ISBN 0-9721314-0-X.