It’s just a soft tissue injury!” the defense attorney scoffs. “They should have gotten better in four to six weeks and our neurosurgeon of twenty-five years will testify to that.”
Does this sound familiar? So what should you do to get around this argument? Well, first of all, you need to perform all tests and exams in the most objective fashion possible and back them up with The AMA Guides to the Evaluation of Permanent Impairment (AMA Guides1) and the Cervical Acceleration/Deceleration (CAD) Injury Guidelines.2 Everything that you perform in the office, (exams, tests…etc), needs to be objective so that it is in a format that is reliable and reproducible and, therefore, becomes a fact. You can perform the subjective tests outlined in the books mentioned above and then back them up with objective tests. For example, if you complete a ROM examination on a patient then back up your findings with a computerized ROM examination utilizing computerized dual inclinometry, you will be the most correct between an independent medical examiner and yourself, because your test is the gold standard, which is computerized dual inclinometry.

The research that the defense attorney’s expert witness refers to the most in their four to six week stance comes mostly from journal articles that refer to healing times with ankle sprains/strains.3 As we all know, the ankle structures are a far cry from the neck structures. But, if you are not going to allow the neck be compared to the ankle, then what can you compare the patient’s injury to so that a jury can make a fair and honest decision. This is where you can utilize the information contained within the AMA Guides. (I like to call this book BJ’s last green book, because it is very conducive to the chiropractic practice).
What do the AMA Guides say about these types of soft tissue injuries? The AMA Guides outline the diagnosis related estimates (DRE) method in tables 15-3, 15-4 and 15-5 and they state that a loss of motion segment integrity or alteration of motion segment integrity (AOMSI) is considered a category IV impairment, the second highest category, and is equal to a 25-28 percent impairment of the cervical, 20-23 percent impairment of the lumbar spine and a 23-25 percent impairment of the thoracic spine. The significance of DRE category IV is that it also contains a 50 percent compression fracture of a vertebral body. So, to say; “It’s just a soft tissue injury,” reveals how uneducated and/or ignorant the person is on human biomechanics and anatomy. Because the over 200 doctors on the front of the AMA Guides consider that a 50 percent compression fracture is a serious injury and they placed AOMSI in the same category, therefore, they also consider AOMSI a very serious injury.

So, how do you measure for AOMSI? The AMA Guides state how to evaluate for AOMSI on pages 378-379. However, I would not stop there, because the explanation states how to perform the evaluation on the radiographs by hand. This is not the most objective marking scheme because marking radiographs by hand has a 26 percent error rate, according to Siegler and Howe.4 This is not the type of evidence you want to be sitting on the witness stand with while a seasoned defense attorney hammers you with one of your diagnostics tests that has a 26 percent error rate. Therefore, to make the marking scheme outlined in the AMA Guides truly objective, you need to have the radiographs digitized and a biomechanical analysis performed on them. This will provide you with the objective evidence of whether or not that the patient is injured and how injured he or she is.
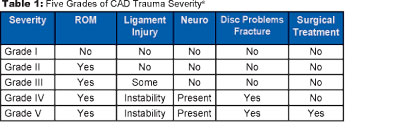
The importance of knowing whether or not that there is significant ligamentous trauma to the spine (cervical, thoracic or lumbar) extends to designing a treatment plan for the patient. The treatment plan that you design for the patient can also be objective in nature when you utilize objective diagnostic tools and the CAD Injury Guidelines. For instance, the CAD Injury Guidelines state that, if there is limited ROM, ligamentous instability, neurological symptoms/findings present, then you can place the patient in a Grade IV injury (Table 1) and that corresponds to frequency and duration of care (Table 2) that would be Daily for 2-3 weeks, 3X/week for ~16 weeks, 2X/week for ~12 weeks, 1X/week for ~20 weeks and then would require a possibility of permanent monthly or an “as needed” treatment schedule.

Here is where I would like to reiterate that ALL of the evidence that you gather should be in an objective format (Table 3). Another reason to perform objective testing on your patient is to confirm or deny your diagnosis. Once you perform your subjective exam/test, then you are able to formulate a diagnosis. This is well and good, but we are taught in school that the purpose of the diagnostic test is to confirm or deny your diagnosis. Therefore, it is prudent that you regularly perform diagnostic tests to make sure that the evidence gathered confirms or denies your findings, thus eliminating any opinion on your part, and creates facts.
By creating facts of the case through objective documentation, you create an evidence-based chiropractic practice that documents whether or not injuries have taken place and how severe the injuries are. The evidence gathered also determines that the care rendered was medically necessary and that you treated the patient in accordance with the established guidelines. This creates a situation where you are not worried about depositions and courts appearances because the defense attorney has nothing to question you about as it pertains to the patient because everything is based on a computerized evaluation or a piece of film that cannot be argued with.
References
1. Guides to the Evaluation of Permanent Impairment, 5th Edition, 2001. American Medical Association Press.
2. Whiplash Injuries: The Cervical Acceleration/Deceleration Syndrome, 3rd Edition 2002. Lippincott Williams and Wilkins.
3. Beynnon BD, Renström PA, Haugh L, Uh BS, Barker H. Am J Sports Med. 2006. September;34(9):1401-12.
4. Siegler & Howe, Inter & Intra examiner reliability of the upper cervical marking system JMPT 1985 8 (2):75-80
Dr. Dwight Whynot is a successful full-time private practitioner in Johnson City, Tennessee, and a graduate of Logan College with a bachelor’s degree from Dalhousie University, Nova Scotia, Canada. Dr. Whynot gives license-renewal lectures on Evidence-Based Chiropractic Practices which are promoted by the EBC Seminars and sponsored by Myo-Logic and Spinal Logic Diagnostics. Dr. Whynot also gives license-renewal lectures to the medical community in Tennessee. For questions regarding evidence-based practice procedures, email [email protected]. For 6 and 12 hours CCE license renewal lecture dates and locations call Karl Parker Seminars at 1-888-437-5275 or visit www.EBCSeminars.com.