
:dropcap_open:O:dropcap_close:nce again, our profession is at odds with itself over something whose benefits it should be welcoming with open arms – “spinal decompression”.One of my early mentors told me, “Chiropractors circle the wagons and then shoot at each other.” Today it seems that everyone is an expert on either traction or decompression (the latter wasn’t even taught when 98% of us were in school). Moreover, if you don’t hold an opinion in favor of one or the other, you know nothing. Doctors are well known for naming techniques after themselves, yet decompression, as you will learn, was neither pioneered nor developed by chiropractors. I will receive a lot of heat for this article, but, after 34 years in the profession, I can take it. “You gotta face the music if you wanna lead the band.”
 In school, I was taught that chiropractic was a philosophy, an art, and a science. That paradigm bothered me for 35 years, so I decided to create my own; a new paradigm for the 21st century, and one that remains at the center of all my teaching: “Chiropractic is a science that has an art and embraces a philosophy.”
In school, I was taught that chiropractic was a philosophy, an art, and a science. That paradigm bothered me for 35 years, so I decided to create my own; a new paradigm for the 21st century, and one that remains at the center of all my teaching: “Chiropractic is a science that has an art and embraces a philosophy.”Before I continue, I’d like to make it clear that I make no claims to being the ultimate authority on either decompression or chiropractic. I am a student of both, and shall be for the rest of my life. There is, however, one thing that I am the world’s greatest expert on, and that is me. I believe with every cell in my body that decompression is working wonders for our profession. It has done for chiropractic what cosmetic dentistry did for dentistry. Never before in our history would patients from all over the country — regardless of their insurance coverage — pay cash for a service. “But,” I hear you ask, “isn’t it controversial?” I don’t think so; but there will always be naysayers ready to create controversy, even if it hurts our profession.
The Facts
The amount of money spent on the treatment of low back pain is staggering. Back pain is a billion dollar industry. In 2005, according to Karen Springer in her Newsweek article “The Price of Pain”, Americans spent $85.9 billion looking for relief from back and neck pain through surgery, visits to the doctor, X-rays, MRI scans and medication; that’s up from the 1997 figure of $52.1 billion, as recorded in the Feb 13 1997 issue of the Journal of the American Medical Association (JAMA).
Ms. Springer went on to report, “Not only are more people seeking treatment for back pain, but the price of treatment per person is also up. In the JAMA study, researchers at the University of Washington and Oregon Health & Science University compared national data from 3,179 adult patients who reported spine problems in 1997 to 3,187 who reported them in 2005 — and found that inflation-adjusted annual medical costs increased from $4,695 per person to $6,096. Spinal patient costs were also significantly higher than for nonspinal patients. ‘People with back problems cost 76 percent more on average, than people without back problems each year,’ says study co-author Brook Martin, a research scientist at the University of Washington. “
A research study by Binod Prasad Shaw, MD of Albert Einstein Medical College and Michele K. Shaufele, MD of Emory University states: “In recognition of the extreme burden and impact that musculoskeletal disorders have on society, the United Nations and the World Health Organization (WHO) have designated 2000-2010 as the bone and joint decade.” The study goes on to report that 10 million Americans are currently disabled due to back pain.
So, we know the sums of money involved are staggering but where do we go from here? It would be folly to let the medical world take over decompression while we fight amongst ourselves. Who better to treat disc injuries than today’s chiropractor? In a nation where back pain has reached epidemic proportions, is there a better way, a cheaper way? In her Newsweek article, Ms. Springer states, “Educating doctors about alternative treatments — even when a patient may be clamoring for high-tech intervention —may be another key to reducing costs and relieving pain. ‘They [patients] can’t order drugs and tests for themselves. Somebody has to be offering them,’ says Dr. Michael Haak, a spine specialist and orthopedic surgeon at Northwestern University’s Feinberg School of Medicine. ‘You need to encourage [doctors and patients] to be aware of all the alternatives.’”
The time for decompression is now. Now is the time to take what we deserve. Yet, we are a profession governed by two associations: the ICA and the ACA. Anyone who knows me knows that I have tried not to be a democrat or a republican. How many other professions have two ruling bodies? It’s time for both associations to recognize that “working as one” would be in the best interests of chiropractors and patients. Our associations should be outraged that physical therapists are paid more for therapy than our doctors.
How do we become experts on anything? We read, we research, we challenge, we acknowledge. To learn, we must be open-minded; those who claim to be “the one and only” are simply attempting to “educate” through insecurity and intimidation.
So where did all this begin? In order to find out, we must go back to the beginning in order to allow you, the educated reader, to draw your own conclusions.
It all began in Ontario in 1987 with Canada’s former minister of health Dr. Allan Dyer. Already recognized as a pioneer in the development of the external cardiac defibrillator, Dr. Dyer designed and developed this new technology to be distinctly different from conventional traction tables. Although traction has been around for centuries, research into its effectiveness remains inconclusive. Dr. Dyer took the concept of traction and made critical engineering improvements to yield a treatment of unprecedented efficacy.
He called his invention Vax-D, (Vertebral Axial Decompression). While Vax-D did manage to overcome many of the limitations imposed by conventional traction, it still had a number of drawbacks. The rigid horizontal table made it difficult for some patients to use, and it was not designed to provide decompression for the neck.
:quoteleft_open:He called his invention Vax-D (Vertebral Axial Decompression).:quoteleft_close:
Although Vax-D could treat the lumbar spine, patients were only able to lie on the table in the prone position. Today Vax-D technology has been reengineered to put the patient in the supine position. The people who attack Vax-D would doubtless have attacked Henry Ford when he altered the Model T. Technology has advanced at a rapid pace, from our computers to our televisions. Old-schoolers never want to change; they fail to see that change is the only constant thing in life.
Numerous studies have been carried out on spinal decompression. To me, a decompression table is only as good as its research results. When teaching decompression, I urge my students to read, understand and embrace the research. One of the first and largest available studies on the efficacy of non-surgical disc decompression was the data compiled by Gose, Naguszewski and Naguszewski and published in Volume 20 of the journal Neurological Research. The data presented the outcomes of 778 patients from 22 medical centers. These patients had had pain for an average of 40 months. Thirty-one of them had previously undergone low back surgery. The treatment consisted of 10 to 20 treatment sessions. Six patients were excluded from the study because they improved before 10 treatments.
- 34 patients had extruded discs.
- 195 had multiple disc herniations.
- 382 had single disc herniations.
- 147 had degenerative discs without herniations.
- 19 had facet (joint) pain.
- 31 of these 778 patients had previous low back surgery.
The Results Were Extraordinary
- 1% reported increased pain.
- 7% reported no change.
- 92% reported improvement. Of these, 5% improved by 25-50%; 17% improved by 50-75%; 70% improved by 75-100%.
- Before treatment, on a pain scale of 0–5, the average pain for all subjects was 4.1. After treatment it was 1.2—a difference of 71%.
- 71% reported that their pain reduced to 0–1 on the 0–5 pain scale.
- Extruded disc patients reported an average 56% reduction in pain and 53% reported that pain reduced to 0–.
- Multiple herniated disc patients reported a 71% reduction in pain and 72% reported that pain reduced to 0–1.
- Single herniated disc patients reported a 71% reduction in pain and 73% reported that pain reduced to 0–1.
- Degenerative disc disease patients reported a 70% reduction in pain and 72% reported that pain reduced to 0–1.
- Facet syndrome patients reported a 72% reduction in pain and 68% reported that pain reduced to 0–1.
- Of patients who had reported decreased spinal mobility before treatment, 77% reported improved spinal mobility.
- Of patients who had reported limited activities before treatment, 78% reported improved activities.
On a scale of 0–3, the average level of satisfaction with treatment was 2.4, in other words, “very satisfied” to “completely satisfied” with their treatment.
This prestigious study paved the way for the use of spinal decompression.
Although research was and has been positive, many insurance companies concluded that these statistics were misleading and inconclusive. Study after study showed the efficacy of spinal decompression but whenever these positive studies appeared, there was always a naysayer on hand to find fault.
Clinical Research
The numerous studies that have been conducted on decompression therapy have consistently upheld its efficacy.
1. Sherry E, Kitchener P, and Smart R, “A prospective randomized controlled study of VAX-D and TENS for the treatment of chronic low back pain.” Journal of Neurological Research, Vol. 23, October 2001. A randomized study which compared VAX-D to transcutaneous electrical nerve stimulation (TENS) in the treatment of patients with chronic (> 3 months in duration) low back pain. Successful outcome was defined as a 50 % decrease in pain using the Visual Analog Pain Scale and an improvement in the level of functioning as measured by patient-nominated disability ratings. The TENS-treated group (n = 21) reported a success rate of 0%, while the group treated with VAX-D (n = 19) showed a success rate of 68.4 %. In spite of this positive finding, Blue Cross reported, “While a 68% success rate was associated with VAX-D compared to a 0% success rate associated with TENS therapy, without a true placebo control, the results are difficult to interpret scientifically.”
Let’s face it; insurance companies have no desire to pay anything to anyone. I can accept the fact that they don’t consider spinal decompression therapy to be reimbursable but, as professionals, we do not need the approval of the insurance companies; the important thing is to continue with the research.
The medical community has provided countless studies that have showed the efficacy of spinal decompression, and while our profession openly and subjectively debates it, modern medical journals have documented its success. I have the opportunity to work with developers, inventors, and engineers while studying the materials and protocols of Dr. Norman Shealy in detail. Norman Shealy in detail. Dr.Shealy, MD, PhD, a former Harvard Professor who has more published articles than any other doctor in our nation On Spinal Decompression, published a review of over 50 traction device studies which led to his identification of mechanisms of action improvements. His observations resulted in the development of the first targeted angle approach by implementing the fixed tower, which, in my opinion, is germane for an accurate angle of pull. Researchers and engineers have confirmed this. His use of the fixed tower in the original DRS system boosted outcomes significantly above the 68% success rate of Vax-D. The DRS patented by Shealy-Becerra, et al. demonstrated an 82-86% success rate. In 2001 the Spina/Accu-Spina IDD Therapy systems further advanced multiple patented technologies which contributed to those device studies, and raised the bar yet again. In the McClure study, carried out by neurosurgeon Dr. Dennis McClure, over 500 patients cleared for spinal surgery were instead given spinal decompression utilizing IDD Therapy. This resulted in 92% of participating patients being able to avoid surgery, and to report continued relief even after the one year follow up period. Medical research has determined the efficacy of spinal decompression. We as chiropractors need to embrace this research and I challenge each and every chiropractic school to begin doing so today.
Additional reading and areas for further research:
Eyerman E, “MRI Evidence of Mechanical Reduction and Repair of the Torn Annulus Disc.” International Society of Neuroradiologists, October 1998; Orlando.
Shealy, C Norman and Borgmeyer V, “Decompression, Reduction and Stabilization of the Lumbar Spine: A Cost-Effective Treatment for Lumbosacral Pain.” AJPM, 1997.
Dr. C. Norman Shealy, MD, PhD, and Vera Borgmeyer, RN, MA, iconic figures in the field of decompression, reported the following:
SUMMARY —American Journal of Pain Management Vol. 7. No. 2 April 1997 Emerging Technologies: Preliminary Findings
“We have compared the pain-relieving results of traditional mechanical traction (14 patients) with a more sophisticated device which decompresses the lumbar spine, unloading of the facets (25 patients). The decompression system gave ‘good’ to ‘excellent’ relief in 86% of patients with RID and 75 % of those with facet arthroses. The traction yielded no ‘excellent’ results in RID and only 50% ‘good’ to ‘excellent’ results in those with facet arthroses. These results are preliminary in nature. The procedures described have not been subjected to the scrutiny of review nor scientific controls. These patients will be followed for the next six months, at which time outcome-based data can be reported. These preliminary findings are both enlightening and provocative. The DRS system is now being evaluated as a primary intervention early in the onset of low back pain especially in workers’ compensation injuries.”
Tilaro F, “An Overview of Vertebral Axial Decompression.”
Naguszewski W, Naguszewski R and Gose E, “Dermatomal Somatosensory Evoked Potential Demonstration of Nerve Root Decompression after VAX-D Therapy.” Journal of Neurological Research, Vol. 23, October 2001.
Ramos G and Martin W, “Effects of Vertebral Axial Decompression on Intradiscal Pressure.” Journal of Neurosurgery,1994.
Shealy C Norman and Leroy P, “New Concepts in Back Pain Management: Decompression, Reduction, and Stabilization.”
Pain Management: A Practical Guide for Clinicians, Vol. 1, 1998.
Tilaro F and Miskovich D, “The Effects of Vertebral Axial Decompression on Sensory Nerve Dysfunction.” Canadian Journal of Clinical Medicine, January 1999.
In his article on the subject of traction versus decompression, Dr. Alan Presswood states the following: “Traction is designed to try to take pressure off the nerves, period. Spinal decompression is designed to relieve pressure and heal the disc so the patient can perform normal movement in the area once again without fear of the problem returning.” The Shealy, Borgmeyer, study confirms this difference based on quantifiable results.
So what do you do? Where do you go from here? Don’t just put a table into your office to make more money; focus on results, embrace the research. When looking to get into the decompression business, do your homework and make an educated decision.
Dr. Eric S. Kaplan, a former President COO of a NASAQ traded public company, which included Nutrisystem, Currently he is CEO of Concierge Coaches, Inc., www.conciergecoaches.com, a comprehensive coaching firm with a successful, documented history of assisting doctors create profitable practices nationwide, providing over 30 New Patient marketing Programs. Dr. Kaplan is a member of the adjunct faculty at Parker. Parker University now offers a National Certification course on spinal decompression. For more information on coaching or spinal decompression, call 1-561-626-3004.
 Following recent publication of a rat study that indicated differences in gut microbial concentrations at the time of type 1 diabetes onset, the authors designed a small human study to test their hypothesis that type 1 diabetes in humans could also be linked to specific microbes in the human gut.
Following recent publication of a rat study that indicated differences in gut microbial concentrations at the time of type 1 diabetes onset, the authors designed a small human study to test their hypothesis that type 1 diabetes in humans could also be linked to specific microbes in the human gut.
 This paper, a 2012 study from Spine, examined the relationship between posture and spinal pain in young people. The authors looked at 1,196 Flemish adolescents. The average age of the 639 male participants was 12.6 years; it was 10.6 years for the 557 females. The authors acknowledge that data relating posture to pain, particularly in young people, are “sparse.” As a profession, chiropractors historically have placed a great deal of emphasis on the relationship between spinal structure and spinal pain, although that emphasis has waned in recent decades. In spite of our profession’s history, a number of previous studies, several of which looked at the status of the spinal curves, have failed to show any clear correlation between posture and spinal pain. Other studies that focused more on regional or segmental misalignment have also failed to show a correlation between spinal structure and pain.
This paper, a 2012 study from Spine, examined the relationship between posture and spinal pain in young people. The authors looked at 1,196 Flemish adolescents. The average age of the 639 male participants was 12.6 years; it was 10.6 years for the 557 females. The authors acknowledge that data relating posture to pain, particularly in young people, are “sparse.” As a profession, chiropractors historically have placed a great deal of emphasis on the relationship between spinal structure and spinal pain, although that emphasis has waned in recent decades. In spite of our profession’s history, a number of previous studies, several of which looked at the status of the spinal curves, have failed to show any clear correlation between posture and spinal pain. Other studies that focused more on regional or segmental misalignment have also failed to show a correlation between spinal structure and pain. 
 At the six-week interval, the patient received a letter from AllFarm Insurance Company stating that an IME has been ordered to determine the necessity of care. The patient showed up at the appointed time for the examination with a friend who joined him during the examination and handed the IME doctor a copy of the MRI on a disc and submitted for examination. The IME doctor spent a total of four or five minutes with the patient, which included the time he spent obtaining the history and doing a physical exam. He released the patient from the examination by walking out in front of the patient and never seeing him ambulate. Two weeks later, the patient and treating doctor received letters from the carrier stating that all future benefits were denied and three out of the six previous weeks’ benefits were denied as well. Upon request of the IME doctor’s report, the treating doctor and patient found the IME doctor stated the diagnosis as lumbar spine strain/sprain resolved.
At the six-week interval, the patient received a letter from AllFarm Insurance Company stating that an IME has been ordered to determine the necessity of care. The patient showed up at the appointed time for the examination with a friend who joined him during the examination and handed the IME doctor a copy of the MRI on a disc and submitted for examination. The IME doctor spent a total of four or five minutes with the patient, which included the time he spent obtaining the history and doing a physical exam. He released the patient from the examination by walking out in front of the patient and never seeing him ambulate. Two weeks later, the patient and treating doctor received letters from the carrier stating that all future benefits were denied and three out of the six previous weeks’ benefits were denied as well. Upon request of the IME doctor’s report, the treating doctor and patient found the IME doctor stated the diagnosis as lumbar spine strain/sprain resolved.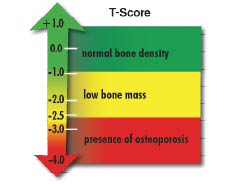
 Increased thoracic kyphosis is associated with osteoporosis and results in a reduced quality of life (QOL). It is also associated with alteration of postural balance, resulting in increased risk of falling. Falls in the geriatric population are associated with increased incidence of fracture.2 Among older adults (those 65 or older), falls are one of the leading causes of injury and death. They are also the most common cause of nonfatal injuries and hospital admissions for trauma. In 2010, 2.3 million nonfatal fall injuries among older adults were treated in emergency departments and more than 662,000 of these patients were hospitalized.3
Increased thoracic kyphosis is associated with osteoporosis and results in a reduced quality of life (QOL). It is also associated with alteration of postural balance, resulting in increased risk of falling. Falls in the geriatric population are associated with increased incidence of fracture.2 Among older adults (those 65 or older), falls are one of the leading causes of injury and death. They are also the most common cause of nonfatal injuries and hospital admissions for trauma. In 2010, 2.3 million nonfatal fall injuries among older adults were treated in emergency departments and more than 662,000 of these patients were hospitalized.3 
 As a full-service Third Party Administration firm (TPA), we welcomed the “full disclosure” of fees promulgated by recent Labor Department regulations. Naïvely, we believed this would open the eyes of plan sponsors to the exorbitant fees charged by the typical mutual-fund sponsored plans, payroll company plans, or any of the other “bundled” plans offered by many in the financial advisory community. Sadly, the disclosures were done in such a way that few took notice.
As a full-service Third Party Administration firm (TPA), we welcomed the “full disclosure” of fees promulgated by recent Labor Department regulations. Naïvely, we believed this would open the eyes of plan sponsors to the exorbitant fees charged by the typical mutual-fund sponsored plans, payroll company plans, or any of the other “bundled” plans offered by many in the financial advisory community. Sadly, the disclosures were done in such a way that few took notice.
 :dropcap_open:I:dropcap_close: talk to a lot of chiropractors across the country. My business, Matlin Manufacturing Inc., brings me into contact with doctors with a wide range of backgrounds and techniques. The number of techniques and therapeutic modalities used by chiropractors is extremely varied. Almost without exception, the vast majority of chiropractors I’ve spoken with still center much of their treatments for spinal pain around the use of spinal manipulation. Manual manipulation of the spine is most often rendered in the form of high-velocity/low-amplitude (HVLA) adjustments. So in spite of all the observed differences between chiropractors of varying backgrounds, this one commonality seems to remain for the majority of doctors.
:dropcap_open:I:dropcap_close: talk to a lot of chiropractors across the country. My business, Matlin Manufacturing Inc., brings me into contact with doctors with a wide range of backgrounds and techniques. The number of techniques and therapeutic modalities used by chiropractors is extremely varied. Almost without exception, the vast majority of chiropractors I’ve spoken with still center much of their treatments for spinal pain around the use of spinal manipulation. Manual manipulation of the spine is most often rendered in the form of high-velocity/low-amplitude (HVLA) adjustments. So in spite of all the observed differences between chiropractors of varying backgrounds, this one commonality seems to remain for the majority of doctors. 
 In addition to the possible mistakes that can be made on the CMS-1500 claim form, you have to consider what potential problems can arise after you have verified a patient’s insurance coverage and benefits. Even after all the correct steps have been followed carefully in the verification process and you have received a verbal and written explanation of benefits, claims can still be denied for payment due to an error on the carrier’s part. When you are accepting an insurance assignment and mistakes happen (e.g., errors in copays or deductible amounts, etc.), if it is discovered that patients actually owe more than what they were told they owed and have already paid (as the result of misquoting benefits), chances of collecting are often slim. Moreover, it can leave patients with a negative reminder of your financial policies. It sometimes becomes a vicious cycle. It can take weeks to discover if the carrier misquoted benefits and as a result, insufficient (wrong) amounts were collected from the patient. This is one reason why the carrier continually reminds us during every step of the verification cycle that “benefit details are not a guarantee of payment!”
In addition to the possible mistakes that can be made on the CMS-1500 claim form, you have to consider what potential problems can arise after you have verified a patient’s insurance coverage and benefits. Even after all the correct steps have been followed carefully in the verification process and you have received a verbal and written explanation of benefits, claims can still be denied for payment due to an error on the carrier’s part. When you are accepting an insurance assignment and mistakes happen (e.g., errors in copays or deductible amounts, etc.), if it is discovered that patients actually owe more than what they were told they owed and have already paid (as the result of misquoting benefits), chances of collecting are often slim. Moreover, it can leave patients with a negative reminder of your financial policies. It sometimes becomes a vicious cycle. It can take weeks to discover if the carrier misquoted benefits and as a result, insufficient (wrong) amounts were collected from the patient. This is one reason why the carrier continually reminds us during every step of the verification cycle that “benefit details are not a guarantee of payment!”
 The practice of meditation is a self-directed process that shifts awareness to take focus away from the usual conditioning of our minds and thinking, which is often developed through our habits and usually without conscious intent. When the mind becomes quiet through meditation, a quiet stillness arises from the balance of body, mind, and spirit that, in turn, relaxes our nervous system. When we tap into our inner power by meditation, we can experience a transformation of the body, mind, and spirit.
The practice of meditation is a self-directed process that shifts awareness to take focus away from the usual conditioning of our minds and thinking, which is often developed through our habits and usually without conscious intent. When the mind becomes quiet through meditation, a quiet stillness arises from the balance of body, mind, and spirit that, in turn, relaxes our nervous system. When we tap into our inner power by meditation, we can experience a transformation of the body, mind, and spirit.
 Elastic therapeutic taping has taken off in the United States as an exciting addition to the manual therapist’s treatment toolbox. Since the 2008 Olympics, a slew of elastic tapes have made their way onto the market, touting their therapeutic benefits. As a Certified Kinesio Taping® Instructor (CKTI), I have learned that each brand of elastic therapeutic tape shares some of the properties of Kinesio Tape, but no other tape shares all of its properties. As the properties of each tape are unique—variations include thread count in the material, the degree of elasticity, the amount of recoil and the amount and quality of adhesive—one cannot generalize application methods across brands of elastic therapeutic tape. Each brand must be used in a way that is appropriate for the target population and with application methods designed for its particular properties. My goal here is to educate the reader specifically about the KTM and demystify its particular therapeutic effects.
Elastic therapeutic taping has taken off in the United States as an exciting addition to the manual therapist’s treatment toolbox. Since the 2008 Olympics, a slew of elastic tapes have made their way onto the market, touting their therapeutic benefits. As a Certified Kinesio Taping® Instructor (CKTI), I have learned that each brand of elastic therapeutic tape shares some of the properties of Kinesio Tape, but no other tape shares all of its properties. As the properties of each tape are unique—variations include thread count in the material, the degree of elasticity, the amount of recoil and the amount and quality of adhesive—one cannot generalize application methods across brands of elastic therapeutic tape. Each brand must be used in a way that is appropriate for the target population and with application methods designed for its particular properties. My goal here is to educate the reader specifically about the KTM and demystify its particular therapeutic effects.