
 :dropcap_open:I:dropcap_close: talk to a lot of chiropractors from all across the country. My business (Matlin Mfg. Inc.) brings me into contact with doctors from a very wide range of backgrounds and techniques. The number of techniques and therapeutic modalities used by chiropractors is extremely varied. But almost without exception, the vast majority of chiropractors still center much of their treatment for spinal pain around the use of spinal manipulation. Manual manipulation of the spine is most often rendered in the form of High Velocity/Low Amplitude (HVLA) adjustments. So in spite of all the differences we might observe between chiropractors of differing backgrounds, there remains this one thing which the vast majority of us seem to have in common.
:dropcap_open:I:dropcap_close: talk to a lot of chiropractors from all across the country. My business (Matlin Mfg. Inc.) brings me into contact with doctors from a very wide range of backgrounds and techniques. The number of techniques and therapeutic modalities used by chiropractors is extremely varied. But almost without exception, the vast majority of chiropractors still center much of their treatment for spinal pain around the use of spinal manipulation. Manual manipulation of the spine is most often rendered in the form of High Velocity/Low Amplitude (HVLA) adjustments. So in spite of all the differences we might observe between chiropractors of differing backgrounds, there remains this one thing which the vast majority of us seem to have in common.I’ve also noticed one more thing chiropractors tend to have in common. As a group, chiropractors tend to not be lacking at all in confidence as to the value of their adjustments. By far, most chiropractors tend to strongly ‘believe” in the value of the adjustment. And most of the time, that’s probably a good thing. This month’s covered article supports the value of your adjustments compared to medications and home exercise. But beyond the author’s published conclusions, I think you might find this paper thought provoking in terms of where the profession (and your practice) may be headed in the future.
The Facts:
- This study examined 272 patients (ages 18-65) who suffered from neck pain for two-twelve weeks.
- Patients were randomly assigned into one of three treatment groups which received either spinal manipulative therapy (SMT), medication (M) or home exercise (HE) with advice.
- The authors sought to determine the relative effectiveness of the three different types of care for both acute and subacute neck pain in both the short and long term.
- The primary outcome measured in the study was pain. Assessments were made at 2, 4, 8, 12, 26 and 52 weeks using a numerical scale from zero (no pain) to 10 (highest severity).
- Secondary outcomes measured included self reported disability, general satisfaction, use of medications, general health status as reported on a health survey.
- Spinal adjustments (SMT) were “diversified” type manipulation delivered over a 12 week period by experienced chiropractors.
- The specific spinal level to be adjusted was left to the discretion of the provider as determined by “palpation of the spine and associated musculature and the participant’s response to treatment.” Treatment also included advice to “stay active or modify activity” as determined by the practitioner.
- Medical treatment (M) provided by a licensed physician included NSAIDS, narcotics, and/or muscle relaxants as determined to be necessary by the physician.
- Home exercise with advice (HE) was provided in two separate one hour sessions in a university outpatient setting. The program included “simple self-mobilization exercise” of neck and shoulders.
Take Home:
Chiropractic care (SMT) proved most effective than medication both in terms of pain and in most of the secondary outcomes. Home exercise with advice (HE) was a very close second and actually produced “similar short- and long-term outcomes.” In fact, the HE group actually showed the most improvement in terms of spinal motion. Patients in the medication group fared the worst and a number of patients in the M group reported using higher levels of pain medication by the end of the study
Many chiropractors utilize both manipulation and exercise. The authors make note of the limited difference in outcomes for the HE group and took pains to point out that ” the potential for cost savings over both SMT and medication interventions, is noteworthy.”
Obviously it’s neat to have evidence supporting the chiropractic adjustment over NSAIDS, pain meds and muscle relaxers. But readers should take note. This paper also highlights the comparable outcomes and significant cost savings of active care/home care programs. Doctors who fail to provide exercise plans for acute/subacute spinal pain may well find their care plans in the cross hairs as plan administrators look continually to cut costs.
The study also made me consider that all too often pain relief may be the only thing many third parties are paying attention to. Unfortunately, that’s also the case with many chiropractors who simply adjust until patients feel better and then rinse and repeat whenever another exacerbation occurs. If all we do is relieve pain, then we can hardly blame interested third parties for seeking out the cheapest method available. I submit that if the profession hopes to survive and prosper, we are increasingly going to be challenged to show exactly how we produce improved clinical outcomes above and beyond the resolution of pain.
Special thanks to our Chiropractic Sciences Contributor Roger Coleman DC for this interesting article.
Reference:
Bronfort G, Evans R, Anderson AV, Svendsen KH, Bracha Y, Grimm RH. Spinal manipulation, medication, or home exercise with advice for acute and subacute neck pain: a randomized trial. Ann Intern Med. 2012;156(1 Pt 1):1-10.
Link to Abstract: http://www.ncbi.nlm.nih.gov/pubmed/22213489
Dr. Mark R Payne, Phenix City, AL is Editor of ScienceInBrief.com, a scientific literature review for busy chiropractors. He is also President of Matlin Mfg Inc. a manufacturer of postural rehabilitation products since 1988. Subscription to ScienceInBrief.com is FREE to doctors of chiropractic and chiropractic students. Reviews of relevant scientific articles are emailed weekly to subscribers.

 Evidence-based medicine is the idea that current scientific evidence can be combined with the clinician’s expertise, as well as the patient’s preferences and expectations, to obtain the best outcomes.
Evidence-based medicine is the idea that current scientific evidence can be combined with the clinician’s expertise, as well as the patient’s preferences and expectations, to obtain the best outcomes.
 :dropcap_open:I:dropcap_close:t’s common for patients to come to our office with complaints related to ‘working out’ or ‘over-training’ and not enough rest and recovery in between workout sessions. I see clients involved with athletic pursuits like cross fit, yoga, martial arts, running 5 K’s, swimming, biking, and/or other sports. We have such extremes in the population, those who sit way too much and wind up getting dehydrated and inhibited glutes from excessive and prolonged sitting (they never get physical activity), and those who are exercise ‘junkies.’ I think it’s important as part of the patient history for doctors to question clients about there past and current exercise routines and programs. My hope is that you are able to provide knowledge and have the ability to write exercise programs for home, or at-the-gym sessions for patients in a way that allows for recovery and (high) performance.
:dropcap_open:I:dropcap_close:t’s common for patients to come to our office with complaints related to ‘working out’ or ‘over-training’ and not enough rest and recovery in between workout sessions. I see clients involved with athletic pursuits like cross fit, yoga, martial arts, running 5 K’s, swimming, biking, and/or other sports. We have such extremes in the population, those who sit way too much and wind up getting dehydrated and inhibited glutes from excessive and prolonged sitting (they never get physical activity), and those who are exercise ‘junkies.’ I think it’s important as part of the patient history for doctors to question clients about there past and current exercise routines and programs. My hope is that you are able to provide knowledge and have the ability to write exercise programs for home, or at-the-gym sessions for patients in a way that allows for recovery and (high) performance.
 :dropcap_open:M:dropcap_close:ost of us who have been in practice for a while would probably prefer to think that our accumulated experience must be of some benefit to our patients. Personally, I prefer a bit of experience in some professions… airline pilots for example (I just feel better when I see a gray haired, “Captain Sully” type in the cockpit!). But as you’ll see, experience may not always be the best teacher when it comes to the practice of medicine. This month’s column recaps our review of a 2011 article which sought to determine how physician experience might impact patient outcomes within a hospital setting. And while we don’t have a comparable study that applies specifically to chiropractic, this study should provide food for thought, especially for those of us who have been in practice for a while. Thanks to our chiropractic sciences contributor Roger Coleman, DC (Othello, WA) for this interesting article. I hope you find it helpful.
:dropcap_open:M:dropcap_close:ost of us who have been in practice for a while would probably prefer to think that our accumulated experience must be of some benefit to our patients. Personally, I prefer a bit of experience in some professions… airline pilots for example (I just feel better when I see a gray haired, “Captain Sully” type in the cockpit!). But as you’ll see, experience may not always be the best teacher when it comes to the practice of medicine. This month’s column recaps our review of a 2011 article which sought to determine how physician experience might impact patient outcomes within a hospital setting. And while we don’t have a comparable study that applies specifically to chiropractic, this study should provide food for thought, especially for those of us who have been in practice for a while. Thanks to our chiropractic sciences contributor Roger Coleman, DC (Othello, WA) for this interesting article. I hope you find it helpful.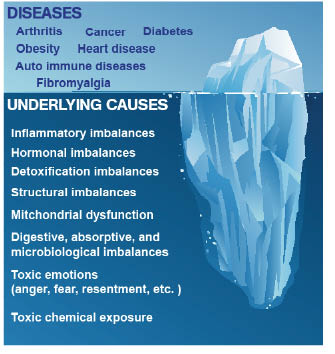
 As the following graphic of an iceberg shows, a named disease such as diabetes, cancer, or fibromyalgia might be visible above the surface, but according to Functional Medicine, the cause lies in the altered physiology below the surface. Usually, the cause of the disease and its symptoms is an underlying dysfunction or an imbalance of bodily systems.
As the following graphic of an iceberg shows, a named disease such as diabetes, cancer, or fibromyalgia might be visible above the surface, but according to Functional Medicine, the cause lies in the altered physiology below the surface. Usually, the cause of the disease and its symptoms is an underlying dysfunction or an imbalance of bodily systems.
 D.D. Had It Right
D.D. Had It Right
 Title:
Title: 
 Difficulty getting up and being fully awake in the morning, even after a full night’s sleep
Difficulty getting up and being fully awake in the morning, even after a full night’s sleep
 What do these terms mean exactly? The vast majority of chiropractors across the globe schedule their patients (adults and children) for their monthly maintenance adjustment visit. We tell our patients that their monthly visit will help prevent and alleviate many problems that they will experience if they do not heed our warnings and accept our preventative-measure philosophy.
What do these terms mean exactly? The vast majority of chiropractors across the globe schedule their patients (adults and children) for their monthly maintenance adjustment visit. We tell our patients that their monthly visit will help prevent and alleviate many problems that they will experience if they do not heed our warnings and accept our preventative-measure philosophy. 
 A cancer diagnosis is terrifying.
A cancer diagnosis is terrifying.