:dropcap_open:I:dropcap_close:n 1999 I was introduced to the Kinesio Taping® Method (KTM) against my will. I was working in rehab in New York City at the time, and a co-worker who had signed up for a course in Massachusetts that included Kinesio Taping had dropped out. My boss asked me to take her place mostly because I had a car and could drive the other two therapists who had signed up. I went grudgingly and with no expectations, as I had never heard of Kinesio Taping. Flash forward to today: I am teaching more than 20 seminars a year and writing about Kinesio Taping for the benefit of my colleagues. You just never know where life is going to take you.

Elastic therapeutic taping has taken off in the United States as an exciting addition to the manual therapist’s treatment toolbox. Since the 2008 Olympics, a slew of elastic tapes have made their way onto the market, touting their therapeutic benefits. As a Certified Kinesio Taping® Instructor (CKTI), I have learned that each brand of elastic therapeutic tape shares some of the properties of Kinesio Tape, but no other tape shares all of its properties. As the properties of each tape are unique—variations include thread count in the material, the degree of elasticity, the amount of recoil and the amount and quality of adhesive—one cannot generalize application methods across brands of elastic therapeutic tape. Each brand must be used in a way that is appropriate for the target population and with application methods designed for its particular properties. My goal here is to educate the reader specifically about the KTM and demystify its particular therapeutic effects.
Having graduated from physical therapy school in 1979, I remember well what a fertile time that was for the growth of manual medicine in the physical therapy profession. I am old enough to have taken a Cyriax course with James Cyriax, a Mennell course with John Mennell, a Strain and Counterstrain course with Laurence Jones, and so on. John Barnes was just coming into his own as the defender and promoter of myofascial release, originally an osteopathic manual treatment, which Barnes has, to his credit, elevated to high art and big business. Back then arguments raged between the stars of manual medicine as to whether it was the disc or the facet joint that was the primary perpetrator of spine-related pain; although, the treatment protocols from the warring camps were not at all dissimilar. Research on manual medicine proliferated from the 1980s on. This was also a time in medicine when specialization was taking over the profession. The specialist was in and the generalist was out: a fact of life that endures to this day. But while all this was going on in the United States and Europe, something truly remarkable happened in Japan in 1979. Dr. Kenzo Kase, an American-trained Japanese chiropractor, introduced a completely original treatment technique that was not orthopedic per se but that had vast orthopedic applications. He advanced a revolutionary concept and modality of treatment based on a non-reductionist concept of how the human body works. Dr. Kase was not interested in addressing parts and pieces of the human organism and healing the individual tissue. His idea was to use tape as a second skin to influence the sensory motor loop between the skin and the brain, creating vasomotor, neuromuscular and neurofascial changes in order to bring stressed tissues throughout the body back to homeostasis. In simple terms, by repositioning the skin over an injured tissue, sensory feedback is transmitted to the brain, which adapts and changes all the tissues in response. In other words, the body heals itself.
Since its introduction to the world market at the 1988 Seoul Olympics, the KTM has taken off as the go-to modality of choice for healthcare practitioners who want to offer their patients both symptomatic relief and resolution of the underlying dysfunction. Please note that I do not use the phrase “pain relief” but rather “symptomatic relief.” The KTM addresses the dysfunctions that occur within the major physiological systems that can lead not only to pain, but also to edema, pathological movement patterns, gait abnormalities, postural insufficiency, muscle imbalance, changes in muscle tone, abnormal scar formation and adhesions and fascial tissue restrictions. As I tell students in my KTM workshops, if you gave me the choice of only one modality to use in addition to my manual treatment and therapeutic-exercise prescription, it would be Kinesio Tape. I can do more with one roll of tape than I can with any ultrasound or stim unit, hot or cold pack, cold laser (although, I really like the cold laser), and so on. All of these modalities have their uses, but none of them can address the myriad issues that Kinesio Tape can.
For those of you who are unfamiliar with Kinesio Tape and the KTM, the tape is adhesive, flexible, stretches longitudinally and was consciously designed to mimic the qualities of skin. It is roughly the same thickness as skin, stretches between 40% and 60% of its resting length, recoils to its original length and is porous. The tape itself is 100% cotton, and the adhesive, which is applied in a wavelike pattern similar to the human fingerprint, is acrylic and heat activated. It can be worn for three to five days and maintain its therapeutic benefit. As there is no latex in the product, the incidence of skin reaction is low.
The underlying theory that led Dr. Kase to invent the tape more than 30 years ago was based on his profound understanding of how the human body works. Each physiological system is dependent on every other system to function and remain healthy. Dr. Kase recognized that the skin and brain communicate constantly to regulate the body’s responses to its internal and external environments. The skin and brain are connected not only by the nervous system, but also by the fascial system, which communicates information from tissue structure to tissue structure at much greater speeds than the nervous system. Therefore, Dr. Kase reasoned that by introducing specific and targeted proprioceptive and neural input through the skin, it was possible to affect physiological systems to change motor output, affect circulation, create or direct fascial movement and modulate pain. If one physiological system could be affected, the other systems would adjust in response. As a practicing chiropractor, Dr. Kase saw how he could affect physiological systems with his hands. He designed the tape to be an extension of his manual treatment so that the work he started with his patients in the clinic could continue at home.
By manipulating the amount and direction of stretch in the tape as it is laid down, its effect can be either compressive or decompressive to the skin and underlying tissues, facilitory or inhibitory to the muscles, optimizing or restricting to motion. Just as force generated by our hands can influence body tissue with such techniques as PNF, strain and counterstrain, and myofascial release, so too can force generated by tape influence tissue.
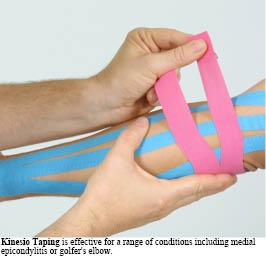
:dropcap_open:Because the tape is on a stretch when it is adhered to the skin, the recoil of the tape moves and lifts the skin…:quoteleft_close:
Because the tape is on a stretch when it is adhered to the skin, the recoil of the tape moves and lifts the skin, creating visible convolutions. These convolutions create a positional change to which the body responds in several ways. First, there is a lymphatic effect and an immediate vascular change. Because the skin is lifted, filaments from the skin attached to the superficial lymphatic vessels pull on the vessel walls, opening the lumen to allow greater volume of fluid flow. Waste products that prolong the inflammatory response are removed more efficiently from the injured tissue, and oxygen-rich blood is introduced to the tissue more rapidly, speeding the healing process. At the same time, the lifting of the skin unloads nociceptors imbedded beneath it, offering immediate pain relief. With movement, the skin wrinkles and relaxes repeatedly, gating the pain on an ongoing basis, much like stroking the skin when one has hurt oneself.
The application of tape to the skin also introduces movement into the fascia, which is connected to skin as well as to every other tissue in the body. Fascia, which has a load-bearing function, is contractile and innervated like muscle. Imbedded within the interstitial tissue are Pacinian and Ruffini bodies sensitive to pressure and vibration, and type lll and type IV fibers, which act as nociceptors, thermoreceptors, chemoreceptors and mechanoreceptors. Tension and pressure activate the mechanoreceptors. Schleip has posited that manual therapy techniques affect these superficial and deep sensory structures, which in turn effect a change in the surrounding fascia and muscle. Plenty of current research supports the position that introducing targeted sensory input manually affects motor output. Kinesio Taping just substitutes the source of the sensory-input change from hands to tape, and, unlike hands, is able to sustain the sensory change for long periods of time.
In specifically addressing pain, Kinesio Taping has an advantage over most other modalities in that it affects more than just the nociceptors. In 2001 Ronald Melzak, Ph.D, proposed a more complex theory of pain than his original gate theory. According to the neuromatrix theory, Melzak suggests, “pain is produced by the output of a widely distributed neural network.” In other words, the pain message is influenced not by nociceptor activity alone, but by multiple pathways. Vision is one example. Seeing a wound or a needle being inserted into one’s skin can enhance the pain experience. We look away to lessen the impact of the pain message. Stress can also enhance the pain experience. Dr. John Sarno, a former orthopedic surgeon who felt that spine surgery was not addressing the cause of most back pain, has made an entire career of diagnosing back pain sufferers with “tension myositis” and treating them with stress reduction. He does very well with it and has saved many people from the surgeon’s knife despite MRI findings that might ordinarily lead to surgery. Psychological and cultural factors also play a role in interpreting the pain message. Some children are trained to be stoic when they are hurt, and some are rewarded by extra attention and treats. The latter group will be more apt to prolong the painful experience to glean the secondary benefits. Likewise, some cultures are generally more stoic and others more emotive, which might color the individual’s perception of pain. Tape addresses not only the nociceptors, but also the patient can see the tape and can psychologically associate it with the positive things happening in therapy. Since the tape can be worn for many days, the visual, psychological and physical effects are ongoing. Placebo is not the main effect of the tape, but it is an element and a good one.
One of the main criticisms I have heard about the tape is that there is no research to support the claims made about its efficacy. My answer to this is that there is overwhelming clinical evidence to prove that Kinesio Taping works to decrease pain and edema to increase proprioception, to assist in postural re-education and to restore normal motor function. The use of this modality has grown to hundreds of thousands of certified practitioners in 80 countries: We cannot all be charlatans or idiots. Research to prove what we see every day in the clinic is starting to be produced but, admittedly, is lacking overall. In the meantime, the findings that have already been published on the effects of manual therapy on the body can certainly be generalized to taping, which is just another way of manipulating soft tissue.
Andrea Wolkenberg, PT, MA, CKTI, has been a practicing physical therapist for more than 30 years. She graduated in 1979 from the University of Pennsylvania’s School of Allied Medical Professions with a Bachelor’s degree in physical therapy. She also holds a Master’s degree in Medical Anthropology in 1986 from the New School for Social Research in New York City. Andrea became a Certified Kinesio Taping® Instructor (CKTI) in 2001. She is currently the Director of Physical Therapy at Spine Options, a pain management center in White Plains, NY, specializing in the conservative treatment of back and neck pain. She is also the President of Spine Solvers Inc., which provides physical therapy services to individuals, injury prevention and workplace safety seminars to businesses, and Kinesio Taping® seminars to health care professionals.