HISTORY
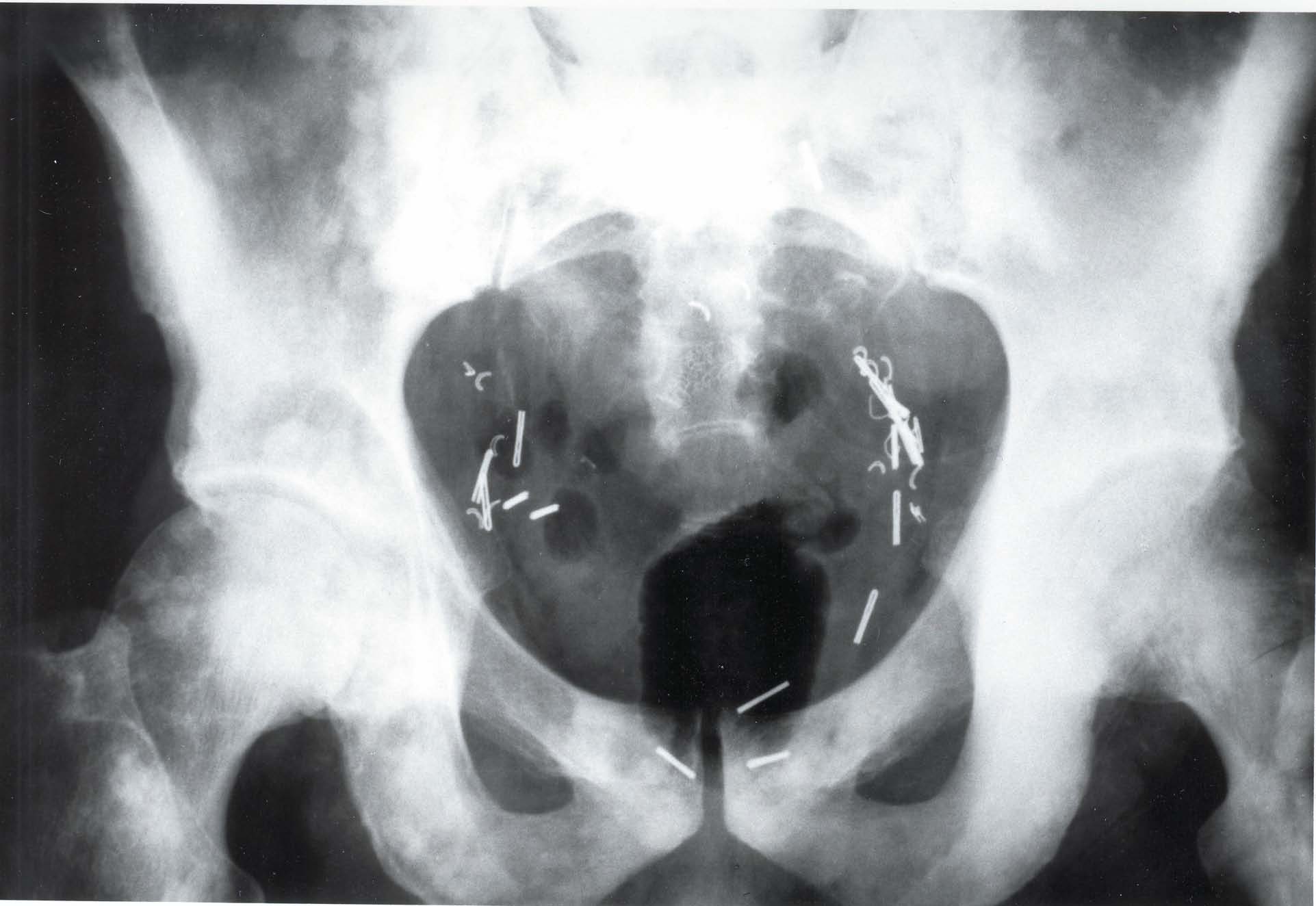
This 60-year-old male patient presents with a history of prostate cancer with surgical removal. Note the metallic clips in the pelvic basin consistent with prostatectomy. There are multiple “snowball” areas of blastic metastasis scattered throughout the pelvis and proximal femora. This radiographic appearance is consistent with osteoblastic metastatic carcinoma from the prostate gland.

DISCUSSION
The sacrum and bones of the pelvis are involved in about 12% of skeletal metastases and may show either lytic or blastic lesions. Seeding from the viscera via Batson’s venous plexus explains this high incidence in the pelvis, as well as in the lumbar spine. Blowout lesions of renal and thyroid origin often affect the bony pelvis. Lesions located in the sacral ala or the posterior ilium are often difficult to perceive on standard radiographs. With the advent of CT scans, a wide variety of lesions involving the osseous pelvis can be more readily seen. The ability of CT to provide accurate measurements of tissue attenuation coefficients and to provide a cross-sectional scan for three dimensional viewing has made it a powerful tool in musculoskeletal diagnosis, with a profound influence on patient management. It provides information about the extent of the bony lesion, localization (for biopsy and radiation therapy), and relationships with other structures. As equipment improves, it seems probable that CT will assume a more primary role in diagnostic evaluation, particularly of the pelvis, where the complexity of bones and the overlying bowel content prevent ideal evaluation with conventional radiographs.
Occasionally, blastic lesions affecting the pelvic rim, especially from carcinoma of the prostate, exhibit an expansion of bone. This occurs as a result of cortical thickening from endosteal or periosteal apposition of bone. The bony enlargement may mimic the appearance of Paget’s disease. Usually, other skeletal lesions are present to assist in radiologic differentiation. Biopsy of the lesion may be necessary as a final step in diagnosis.
Dr. Terry R. Yochum is a second generation chiropractor and a Cum Laude Graduate of National College of Chiropractic, where he subsequently completed his radiology residency. He is currently Director of the Rocky Mountain Chiropractic Radiological Center in Denver, Colorado, and Adjunct Professor of Radiology at the Southern California University of Health Sciences, as well as an instructor of skeletal radiology at the University of Colorado School of Medicine, Denver, CO. Dr. Yochum can be reached at 1-303-940-9400 or by e-mail at [email protected].
Dr. Chad J. Maola is a 1990 Magna Cum Laude Graduate of National College of Chiropractic. Dr. Maola is a Chiropractic Orthopedist and is available for post-graduate seminars. He may be reached at 1-303-690-8503 or e-mail [email protected].