In the 20th century, the electric motor became part of our culture. The creation of intermittent power traction became a reality. This remained unchanged until Dr. Allen Dyer introduced decompression therapy in 1991.1
Dr. Dyer felt that, to reach the inner disc core, traditional traction needed modification.
Although intermittent traction is an effective therapy for elasticity, circulation, inflammation and facet movement, it did not adequately address the internal needs of the disc. In other words, to more effectively treat the intervertebral disc, the pull-release ratios needed to change. Dr. Dyer discovered and developed a unique pull-release pattern that proved more effective to the disc than traditional traction.
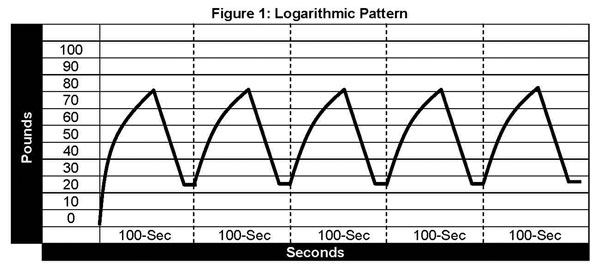
This was the creation of the “logarithmic pattern.” Although it is technically a traction pattern, it is the only traction pattern classified as decompression.
Figure 1 represents the logarithmic pattern. Simply defined, it is a unique 100-second cycle comprised of a 60-second loading of the pull-force, followed by a 30-second unloading of the pull-force, and finishing with a 10-second rest. The cycle repeats itself for the 30-minute session.2

Currently there are as many as 14 decompression systems. About half the systems are manufactured by independent companies. The others are manufactured by “outsource” manufacturers who cosmetically re-badge them to look different and retail under private labels as unique machines.
Pricing for the larger sophisticated systems ranges from $65,000 to $149,000. They all claim superiority but, in many respects, they are the same. However there are some distinct differences you should be aware of.
Pull-Release Forces: All decompression systems create their pull and release forces using one of two available systems. They either use a modified “cable-winch” motor, or the more sophisticated “actuator” motor.
So what’s the difference?
The winch motor system is comprised of a cable wrapped around a spool like a fishing reel. Function wise, the cable-winch provides a satisfactory pull but it has very little control of the release value other than to simply unreel and “let go.”
The actuator motor is a more sophisticated system, comprised of an internal gear attached to a long threaded axel shaft. The gear and shaft provide extreme accuracy in both the pull and the release. In addition, actuator motors can be manufactured with internal sensors that provide feedback to locate the position of the actuator shaft. This means the actuator has the capability of setting its pull-release forces by poundage (like cable systems) and by distance (only actuators can control distance). On a clinical note, patients with elongation limitations, i.e., post surgical, tissue sensitivity or geriatric issues, can be treated more safely using distance values. It is an excellent safety feature that should be consider when researching your system.
Postures: There are three postures currently used in decompression. They include supine, prone and reclined sitting.

Because back pain is generally relieved in a reclined position, the majority of traction systems have been designed to treat patients either prone or supine. As equipment improved, there was little thought that went into improving or changing the reclined posture.
In the 1980’s, manufacturers began to improve their creativity by providing the ability to adjust the location or position of the pull-source. For example, tables with the ability to raise or lower the pull source, or shift the pull source to the left or the right, were introduced. Doctors began to realize that pulling the spine in directions other than straight had clinical advantages.
Flexion-distraction systems modified the pull-source position by adding the ability to move the lower extremities “along with” and “in the same direction” as the pull source. This was accomplished by hinging the source of the pull-force under the pelvis.
However, in 2005, the FDA cleared the first system that could treat the spine in a reclined “sitting posture.” This was the first major change in patient treatment posture since the introduction of traction.
Science has proven that postures affect disc pressure. The vertical bar chart in Figure 2 shows how.
The bio-mechanical theory behind “reclined sitting” is based on vertebral-disc positioning. “When sitting in an upright weight bearing posture, the vertebral bodies are flexed onto the disc. This increases disc pressures more than standing. Therefore, if we can decompress the spine in a reclined “sitting” posture, we can create stronger disc vacuums than supine or prone.3
Simply stated, the postures that create the greatest disc pressures under gravity produce the greatest disc vacuums under decompression.
Range of Motion: Range of motion refers to the motion capabilities of a joint. With respect to spinal decompression, range of motion refers to the ability to adjust and vary the spine’s posture during the decompression. The ability to vary and change the posture of the spine as you decompress the spine changes how and where the pull-forces move through the spine.
Combining spinal range of motion (ROM) with decompression is the newest addition to decompression. The ability to articulate the spine through its ranges of motion adds a new and sophisticated dimension to decompression.
If you are researching range of motion, the following planes need to be included:
• Vertical elongation of the spine,
• Flexion and extension of the spine,
• Lateral flexion of the spine,
• Rotation along the vertical axial plane,
• Translation anteriorly and posteriorly.
ROM features or articulating features provide three methods of treatment.
Pre-Postured decompression: This is where the spine is strategically pre-positioned based on X-ray or MRI to vary and improve the effects of the pull-forces through the spine. It can succeed where straight linear pulling fails.
ROM therapy: This is a therapeutic procedure that involves actively moving the spine through a series of postures while the spine is distracted, to restore or improve spinal ranges of motion.
Antalgic Decompression: This is where the patient is positioned into the posture of “least pain” prior to beginning of the decompression cycling.
Regarding axial rotation, the postures used with conventional Flexion-Distraction tables limit rotation because the patient is lying straight. Conversely, the flexed hip and knee posture of reclined sitting enables 90 degrees of lumbar-pelvis rotation because the posture simulates the lumbar side-posture adjustment.
Conclusion
There are many traction-decompression systems to choose from. With so many systems to consider, you must choose wisely. Look for the following features:
• Are the pull-forces created by actuator?
• Can the pull-forces be set by poundage AND distance?
• Can the ROM features provide at least 10 planes of motion?
• Does the system have “built in” patient safety features?
• Does the system have report writing software?
• Are there research studies on the system?
 David Bass, D.C., LAc, DOM, invented the articulating ROM Antalgic-Trak and is current President of Spinetronics the manufacturer of Antalgic-Trak. You can reach him at [email protected] or visit www.Spinetronics.com.
David Bass, D.C., LAc, DOM, invented the articulating ROM Antalgic-Trak and is current President of Spinetronics the manufacturer of Antalgic-Trak. You can reach him at [email protected] or visit www.Spinetronics.com.