:dropcap_open:H:dropcap_close:ow many times have you heard from an athlete, “Make me run faster!” or “Improve my performance!”? Many athletes would gladly take a little pain for better performance and faster speed. However, ignoring the warning signs of pain can be a no-no! We know that the long-term outcome of living for today and not for the future can lead to chronic and disabling injuries. We have all experienced patients who do not follow our recommendations to reduce their workload, decrease training intensity, reduce the amount of miles they are running, etc. It becomes a mental block for many athletes who tell you they will, but really they won’t. First and foremost, it is not your fault. Unfortunately, many novice athletes think taking a few days off or even reducing their training program will affect their performance, whether they are runners or even football players.
If they don’t take your recommendation and refuse to take some time off for their bodies to heal and recover, then eventually they could develop a serious or chronic injury that begins to affect their  activities and eventually activities of daily living. The following is a commonly used grading scale for measuring the level of overuse-type injuries in runners. This is only a guideline for you to use during consultation, similar to an Oswestry pain scale.
activities and eventually activities of daily living. The following is a commonly used grading scale for measuring the level of overuse-type injuries in runners. This is only a guideline for you to use during consultation, similar to an Oswestry pain scale.
activities and eventually activities of daily living. The following is a commonly used grading scale for measuring the level of overuse-type injuries in runners. This is only a guideline for you to use during consultation, similar to an Oswestry pain scale.- Pain comes on after the run, but does not affect time and/or distance
- Pain occurs during the run, but does not affect time and/or distance
- Pain occurs during the run and is affecting time and/or distance
- Pain is severe enough that patient cannot run
- Pain is severe enough that it affects all activities of daily living
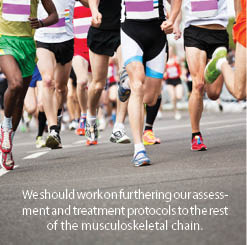
As chiropractors, when we think about increasing the speed of a runner or even a walker, our number-one focus must be on stabilizing any existing vertebral subluxation complexes. We should work on furthering our assessment and treatment protocols to the rest of the musculoskeletal chain. Over the years I have spent a lot of time around the track and listened to numerous high school athletes and track coaches. A popular topic of conversation is about getting the runner to “turn over” his/her stride as fast as possible.
Many drills are done to work on that one phase of running, which means we are talking about power and how quickly we can generate that power. To get a better understanding we must know which muscles come into play to perform this outcome. We know that we increase our power as we go from walking to running to sprinting.
The primary power is generated from the hip extensors during the first half of stance phase, the hip flexors at the time of toe off, the knee extensors during the second half of stance, the ankle plantar flexors just before toe off, along with the hip abductors. (1)
The hamstring and gluteus maximus generate the power to pull the body forward by actively extending the hip after initial contact, when our foot is placed ahead of the body. Then, during the second half of stance phase, the quadriceps and gastrocnemius contract to push us forward by extending the knee and plantar flexing the foot. The hip abductors then contract to provide lift. Finally, the psoas propels the leg into swing phase by flexing the hip.
Thus the total amount of power generated increases as speed increases. The relative contribution from each of these muscle groups changes such that relatively more power is generated proximally (at the hip) as speed increases. (1) Based on this information alone, we must put our focus on a subluxation-free and strong musculature of the hip area.
Making Runners Faster
:dropcap_open:We also know that another leading cause of stride asymmetry is abnormal foot function caused by muscle imbalances.:quoteleft_close:
Ultimately, to make a runner faster two important keys are necessary. The first is the runner must have a consistent stride rate, or symmetrical stride. The second is a symmetrical stride length. The average stride rate ranges between 180-200 strides per minute.
Ultimately, to make a runner faster two important keys are necessary. The first is the runner must have a consistent stride rate, or symmetrical stride. The second is a symmetrical stride length. The average stride rate ranges between 180-200 strides per minute.
Have the runner count his number of steps for 15 seconds and multiply by four. He should do this over several portions of his run to come up with a reasonable average. Then you can determine the speed at which a runner runs by multiplying the steps he takes per second (known as cadence) by the stride length.
To get an accurate measure of stride length I recommend doing what has worked for me for over 25 years – gait analysis using video and computer programs. Regardless of which program you use, it is important to do a follow-up analysis of your patient after a recommended course of care. You should check to see if your recommended treatment plan is improving stride length and improving symmetry in the three phases of the gait cycle. To learn more about what programs I use in my practice, visit my website at www.albionrundoctor.com or you can send a query to [email protected].
Research has shown that the main difference between long and short distance runners is the length of stride and not the rate of stride. (2) The average stride length is 2.5 feet long. So to walk one mile it takes approximately 2,000 steps. A common cause of overuse injuries comes from an abnormal symmetry in a patient’s stride length. Let’s do some math: Our patient is walking a one-mile race. Her right leg stride is 2 feet 3 inches and her stride with the left is 2 feet 5 inches, then, over the period of that mile, the right leg takes 100 steps that are 2 inches shorter. This totals to 200 inches or 16 feet 6 inches of distance variable. Substantial? Absolutely!
As doctors of chiropractic we understand the meaning and importance of symmetry. All joints from the spinal joints to the hip joints must move to their fullest innate potential. If you want to sing the bone-and-joint song, starting with “the foot bone is connected to the ankle bone,” then be my guest! We also know that another leading cause of stride asymmetry is abnormal foot function caused by muscle imbalances.
These imbalances can cause inversion or eversion of the foot and the functional movement patterns of hyperpronation, resulting from an anatomical breakdown of the three arches of the foot. Stabilizing the three arches of the foot with stabilizing orthotics to allow a normal heel-to-toe transfer in walking or a midfoot-to-toe transfer in running is very important. Remember, when recommending stabilizing orthotics, it is important to also recommend appropriate footwear.
A 1980 graduate of Palmer College of Chiropractic, Dr. Kirk Lee is a member of the Palmer College of Chiropractic Post Graduate Faculty and Parker College of Chiropractic Post Graduate Faculty. He has lectured nationwide on sports injuries and the adolescent athlete, and currently practices in Albion, Michigan.
References
-
Guten, G. Running Injuries: “Kinetics Overview”, pg 16. 1997 W.B. Saunders Company
-
Rompottie, K. “A study of stride length in running” International Track and Field: 249-56. 1972

 A tendency to toe out (foot flare)
A tendency to toe out (foot flare)
![Forum [ Your Letters & Emails ]](https://buyersguide.theamericanchiropractor.com/wp-content/uploads/2010/09/Forum.jpg)
 I read with interest the two letters that appeared in your May 2009 issue regarding Personal Injury. Dr. Anonymous raised a few issues but he painted with a very broad brush. More interesting was Dr. Studin’s reply. I quite enjoyed Dr. Studin’s thoughtful, articulate and imaginative article in response to the anonymous and clearly disgruntled DC regarding the PI issue.
I read with interest the two letters that appeared in your May 2009 issue regarding Personal Injury. Dr. Anonymous raised a few issues but he painted with a very broad brush. More interesting was Dr. Studin’s reply. I quite enjoyed Dr. Studin’s thoughtful, articulate and imaginative article in response to the anonymous and clearly disgruntled DC regarding the PI issue.