Why is there so much disagreement in the field of professional foot orthotics? When I read articles and research regarding support of the feet and lower extremities, I am constantly reminded that there are two major camps. Each side seems to make a strong argument. If I tell a podiatrist about the types of orthotics I find to be helpful to my patients, I am told that they are no good, and can’t possibly help any patient. Yet my own clinical experience finds the chiropractic types of orthotics to be very useful. In fact, I have had many successful results in patients who have previously attempted—unsuccessfully—to use the rigid type of orthotic with forefoot posting.
I am still amazed that some people can walk—much less be told they should run—in the traditional, rigid-control orthotics. And I still hear stories from my patients of a podiatrist (or even occasionally another chiropractor) who scoffs at the more flexible orthotics I have provided for them. The two ends of the orthotic spectrum are so different that it seems that someone must be right, thereby making the other doctor completely wrong. So the question is: Who or what is right, and who or what is wrong?
Here’s my assessment of the situation: As is true in many similar controversies concerning the human body, the answer depends on the patient’s needs and the training and focus of the practitioner. The two major approaches to providing orthotics are completely different systems which are not interchangeable, and cannot be compared within the other system. Both have their uses and value for patients.
Differing Viewpoints
Each approach has its own construct, or pattern, which is inherently valid. If you start within the conceptual framework of one orthotic philosophy, you are OK, as long as you stay within its confines. Each procedure begins with a different viewpoint, and continues in a rational, reasonable manner to an end result which is a very different-looking product. In other words, each approach makes sense within itself, but the end product (the orthotic) can’t be reasonably judged using the conceptual basis of the other construct. And, really, it is the final result—the patient outcome—which should be the final determinant. If the orthotic achieves the purpose for which it was designed, and is, itself, the cause of no subsequent problems, then the intervention can be considered successful, and the patient is the beneficiary!
Apples Aren’t Oranges
In Table 1, I have attempted to differentiate the two major orthotic constructs. It is evident that both approaches are inherently valid; each one makes sense when viewed from within its own pattern. To use the concepts of one to evaluate the products of another just won’t work. This viewpoint has allowed me to appreciate the differences and to understand better the rationales for the two very different procedures. To jump across columns or mix concepts just doesn’t work; that’s why you can’t send a weight-bearing image of a foot to a podiatric orthotic lab and expect to receive anything useful (and vice versa). Apples are apples and oranges are oranges; just don’t expect an apple to taste like an orange and you won’t be disappointed!
Table 1. Podiatric and chiropractic constructs for orthotic use
|
|
PODIATRIC
|
CHIROPRACTIC
|
|
Patient’s problem
|
Foot pain
|
Spinal problems
|
|
Biomechanical lesion
|
Poor foot function
|
Inefficient support of spine during stance and gait
|
|
Apparent cause
|
Abnormal foot biomechanics
|
Transmission of abnormal forces to pelvis and spine
|
|
Proposed fix
|
Control excessive pronation
|
Provide extremity support
|
|
Method
|
Maintain subtalar neutral
|
Improve arch/ankle function
|
|
Biomechanical concept
|
Forefoot/rearfoot imbalance
|
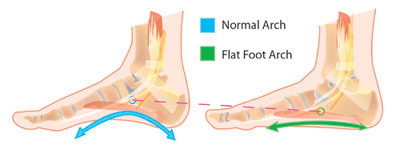
3 arches and heel support
|
|
Orthotic solution
|
Rigid control w/ forefoot & rearfoot posting
|
Flexible support for arches and shock absorption
(occasional rearfoot posting)
|
|
LABORATORY
|
|
|
|
Imaging needed
|
Foot in subtalar neutral (“ideal”) position
|
Foot in functional posture (when it’s providing support for the spine)
|
|
Provider input needed
|
Exact posting measurements
|
Special instructions (lift, etc.)
|
|
Lab procedure
|
Make negative image
|
Take measurements from weightbearing casting
|
|
PROBLEMS
|
|
|
|
Athletes
|
Uncomfortable—often need shock absorption
|
May need more torsional support (i.e,. StanceGuard)
|
|
Orthopedics
|
Problems with compensatory hypermobility
|
Adaptation process may require period of short-term exercise of feet
|
|
Neurological
|
Altered proprioceptive input inhibits postural control
|
Learning period/muscle retraining soreness
|
|
Provider time/expertise
|
Lengthy/high
|
Moderate/moderate
|
|
Patient cost
|
Expensive
|
Moderate
|
|
|
|
|
Dr. John J. Danchik is the seventh inductee to the American Chiropractic Association Sports Hall of Fame. He is the current chairperson of the United States Olympic Committee’s Chiropractic Selection Program, and lectures extensively in the United States and abroad on current trends in sports chiropractic and rehabilitation. Dr. Danchik is an associate editor of the Journal of the Neuromusculoskeletal System, and has been in private practice in Massachusetts for 27 years.