In our March article, we discussed how the physical properties of tight, contracted, paraspinal tissues create resistance to the corrective forces of your adjustments. Last month, I showed you a great example of how one case of scoliosis was successfully managed using simple blocking techniques to introduce sustained stretching forces into the spine. In this article, I want to discuss one effective way to apply the same principles of sustained stretching to correct the cervical lordosis.
Most of your adult patients will present with spines held in sub-optimal postures for many years. The longer your patient has labored under the demands of abnormal posture, the more likely he or she is to have adaptation and contraction of the surrounding soft tissues. Once this occurs, the visco-plastic characteristics of the contracted tissues will sabotage your attempts to adjust the spine back toward normal structure. Shortened and contracted soft tissues simply won’t yield to the rapid on-off forces of traditional adjustments. They require time to stretch. To correct these patients, you need a different tool set.
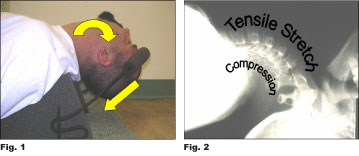
In a previous article, I mentioned that corrective forces should generally be applied for twenty to thirty minutes daily for effective stretch to occur. Two thoughts should leap immediately to your mind here. First, you definitely don’t want to do this by hand and, secondly, it isn’t practical for patients to traction every single day in your office for thirty minutes. If you are really serious about having your patients perform extension traction on a daily basis, much of the work will need to be done at home. There are a number of devices on the market which attempt to restore the lordosis, many of which will work very well. In a shameless act of self promotion, I want to discuss a simple but very effective home traction device manufactured by my company. It’s called the Dakota Traction™ (See Fig.1). Please consider it as just one item for your bag of tricks. Here’s how it works.
One method shown effective in restoring the cervical lordosis is called “extension-compression” traction. So named because the head is extended backward and compressed downward (caudally), the method actually only produces compression loading on the posterior motor units. The anterior motor unit is actually unloaded to create tensile stretch in the anterior soft tissues (See Fig.2). Traction force is provided by a simple, padded elastic band which passes over the forehead. The amount of force can be easily adjusted as needed for patient comfort. In my experience, extension-compression methods are generally well tolerated by about 75 percent of patients. Those patients who find the method uncomfortable may require an alternative method to achieve correction.
Patients generally begin with only a few ounces of force for two or three minutes daily. Patients should gradually increase daily treatment times, as able, until they can comfortably handle twenty to thirty minutes daily. Only after the patient has reached the target time is the traction force increased slightly by tightening the elastic cord. Remember, our goal here is to simply apply gentle stretching force for sufficient time to allow viscous and plastic deformation to take place. I am aware some authorities promote the use of much higher amounts of force to vigorously stretch the neck into lordosis, but I caution all doctors to err on the side of caution here. After all, most of your patients with chronic loss of the cervical lordosis have had their problems for years. It makes no sense to try to hurry the process and, in fact, may be very counterproductive, possibly even dangerous, to do so.

A brief word of caution is appropriate here. Full extension of the head and neck may be contraindicated in certain individuals. Examples of conditions which might increase the risk of complications include, but are not limited to, history of STROKE or cerebrovascular accident, high blood pressure, vertebral/carotid artery disease, diabetes, atheroslerosis, disc protrusion/prolapse, Down’s syndrome, spinal stenosis, spinal fracture or instability, malignancy and/or infection of the cord or column, and advanced osteoporosis. Other symptoms which would contraindicate further use of extension traction methods, particularly if produced or lateralization of pain into the extremities, numbness, paresthesia, muscular weakness, loss of coordination or function, ataxia, visual disturbances, or any other neurological symptoms.
We have developed a suggested protocol to help screen for individuals who may be at higher risk for complications. Although no screening procedure can guarantee safety for any particular individual, it is important we do everything in our power to minimize risk to our patients. I strongly recommend all patients be thoroughly screened prior to treatment. Extension traction procedures have demonstrated a remarkable record of safety for over two decades now. Let’s keep it that way.
Next month I’ll discuss alternatives for patients who simply can’t handle extension-compression traction.
Dr. Mark R. Payne is the president of Matlin Mfg., a manufacturer and distributor of postural rehab products since 1988. To download a full and unabridged version of this article, link to www.MatlinMfg.com. In the meantime, interested doctors should call for a free copy of screening protocol we use in our office. Please call us at 1-334-448-1210 to request your free copy.