The Crossroads of Rehab and Technique
by Mark R. Payne D.C.
Adjusting technique and spinal rehabilitation have always been viewed as two completely separate subjects. Chiropractic’s rich history is replete with innovative ways of adjusting misaligned or dysfunctional spinal segments. Most such chiropractic techniques would be classed as “passive care” in that the patient is a non active recipient of care administered by the doctor.
Rehab, on the other hand, has traditionally been defined as “active care” in that patients become active participants in improving the way their body moves or functions. Rehabilitation typically requires patients to do more than just relax while receiving treatment. Whether the activity is spinal strengthening, cardiovascular exercise, or neuromuscular reeducation, most rehab requires real work by the patient.
For years, the line between technique and rehab seemed very clear. Adjusting technique was basically passive care administered by the doctor, for the purpose of correcting spinal joint dysfunction or misalignment. Rehab has always been defined as activity by the patient for the purpose of improving some aspect of function. Traditionally that makes for a differentiation between the two in the minds of most doctors. But, are we reaching a point where rehab and technique are beginning to overlap when it comes to postural (structural) rehabilitation? Consider the following example.

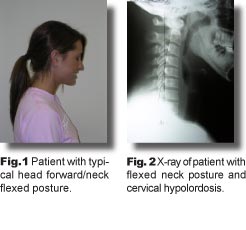
The first two photos show a common postural imbalance and the profound effect on the cervical lordosis. One popular technique teaches drop table adjusting for cervical hypolordosis with the patient placed in the reversed or opposite posture (Fig. 3). The idea here is to maximize the doctor’s efforts at restoring the cervical lordosis by pre-stressing the spine into extension before administering the thrust. Although this adjustment hasn’t proven particularly effective, it serves well for our example here. Most readers would probably agree it falls clearly under the heading of “technique.” This is a manual thrust delivered with the intent of correcting spinal misalignment/subluxation. Sounds like “technique” to me.
But what if we address the same postural misalignment using rehab procedures instead? In Fig. 4 below, the patient performs extension exercise to help restore the lordosis. Here’s a classic rehab procedure, therapeutic exercise, employed for the specific purpose of correcting spinal misalignment. So is it “rehab” or “technique”? On the one hand, it’s certainly active care. On the other hand, our therapeutic goal is now the correction of postural subluxation, a goal traditionally reserved for the adjustment.

Here’s another example. In Fig. 5 the patient performs extension traction of the neck to restore the cervical curve. While not exactly “active” care, the process still requires a level of participation by the patient. Certainly, most doctors wouldn’t classify traction procedures as an adjusting “technique” and yet, the purpose here is exactly the same as that of the traditional chiropractic adjustment, to correct subluxation of the neck.
In fact, some procedures might be better defined by your therapeutic goal than any description of the procedure itself. When patients perform therapeutic exercise to improve muscular function, it’s obviously a rehabilitation procedure. But, when therapeutic exercise is done with an eye toward correcting spinal misalignment, the goal becomes identical to that of many adjusting techniques. Similarly, when patients perform spinal traction for the purpose of symptomatic relief, most of us probably wouldn’t consider it to be part of our “technique.” On the other hand, twenty minutes of extension traction to correct postural subluxation starts to look like more of a slow, sustained adjustment once you consider the real purpose.


Semantics aside, whether or not you view traction or exercise as part of your “technique” may ultimately hinge on your paradigm of what constitutes subluxation. Once you consider subluxation from a postural perspective, it opens the door for new applications of old, standard therapeutic procedures. Try considering other treatment methods from the perspective of improving your patient’s posture as well. How might that change your application of methods like PNF stretching or active release? What about patient education regarding activities of daily living? Or maybe even posture based massage??? Why not! By just stretching your paradigm a bit, you may well find the opportunity to add valuable new tools to your arsenal of corrective care techniques without changing anything about the way you actually adjust your patients.
Dr. Mark Payne is the president of Matlin Mfg., a manufacturer and distributor of postural rehab products since 1988. To learn more about implementing postural rehab into your practice, call 1-334-448-1210 or link to www.MatlinMfg.com to request our FREE REPORT, “The Best Corrections of Your Career.”