In my experience, there is a general lack of appreciation of both the need for radiographic views of the thoracic spine and the influence of the thoracic spine on whole body alignment and health potential. It is for these reasons that I offer this particular series of articles introducing my thoughts on the thoracic kyphosis to readership of the The American Chiropractor.
 Radiographic Measurements
Radiographic Measurements
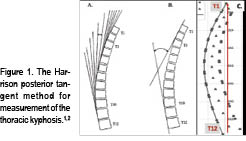
In the early 1980’s, my father–Dr. Donald Harrison1–developed specific radiographic measurement methods to assess the magnitude and distribution of the thoracic kyphosis. These measurements were termed “the Harrison Posterior Tangents.” Later (2001), we investigated the reliability of these kyphosis measures and identified small standard errors of measurement and good to excellent intra- and inter-examiner reliability.2 Figure 1 shows the Harrison posterior tangent method.
Average Thoracic Kyphosis Angles
Several studies have reported “normal” values of thoracic kyphosis in a wide range of age groups.3-5 The density of the upper ribcage, in the coronal plane, can cause an inability to accurately identify and measure the vertebral segments T1-T4. Because of this, various authors have utilized different vertebral levels when measuring the thoracic kyphosis and a large range of values for kyphosis (20° to 50°) has been reported.3,4
 Problematically, some of this normal subject data is contaminated with subjects that should not be considered healthy. For one example, Fon, et al.,5 presented thoracic kyphosis measurement in 316 “normal subjects” aged 2-77 yrs. Their definition of normal was: “…while the general status of some of these patients was not optimal, it was assumed that the patients were sufficiently fit to be ambulatory….”
Problematically, some of this normal subject data is contaminated with subjects that should not be considered healthy. For one example, Fon, et al.,5 presented thoracic kyphosis measurement in 316 “normal subjects” aged 2-77 yrs. Their definition of normal was: “…while the general status of some of these patients was not optimal, it was assumed that the patients were sufficiently fit to be ambulatory….”
Beginning in 2001, my colleagues and I proposed a more narrow distribution of thoracic kyphosis values as normal: average values for T3-T10 posterior tangents = 33°-37°.3,4 Part of our reasoning for a narrower range of normal thoracic kyphosis was based on a study done in 2002.6 Here, we identified that translated postures of the ribcage relative to the pelvis in the sagittal plane can have a strong influence on the magnitude of thoracic kyphosis. Specifically, a total change of 26° in thoracic kyphosis was found for maximum posterior translation of the ribcage to maximum anterior translation in normal subjects. (See Figure 2.)
:dropcap_open:Poorer health status, increased disability, and increased pain levels in patients with anterior trunk postures.:quoteleft_close:
Furthermore, biomechanical models have predicted large increases in extensor muscle loads and consequent increased compression and shear loads on the thoraco-lumbar spine discs when sagittal trunk translation is present.7,8 These high compressive and shear loads may produce pain and initiate or contribute to a degenerative remodeling response in the disc. In fact, Glassman, et al.9, identified poorer health status, increased disability, and increased pain levels in patients with anterior trunk postures.
The issues associated with sagittal plane ribcage translation prompted my colleagues and I4 to present thoracic kyphosis data from a group of 50 normal subjects whose sagittal translation was within 1 standard deviation of the mean (neutral alignment). This data is presented in Table 1.
 Average & Ideal Thoracic Kyphosis Models
Average & Ideal Thoracic Kyphosis Models
 Harrison and colleagues3 presented average geometric models of the thoracic kyphosis (T1-T12, T2-T11, and T3-T10 segments were modelled) as a segment of an ellipse using pooled data from 80 normal subjects’ lateral thoracic radiographs. Figure 3 shows the average elliptical model of the segments T1-T12.3
Harrison and colleagues3 presented average geometric models of the thoracic kyphosis (T1-T12, T2-T11, and T3-T10 segments were modelled) as a segment of an ellipse using pooled data from 80 normal subjects’ lateral thoracic radiographs. Figure 3 shows the average elliptical model of the segments T1-T12.3
Harrison, et al.4 followed this paper with an optimized elliptical model of thoracic kyphosis based in part on data from 50 optimized normal subjects. Since the thoracic vertebral bodies increase in size considerably from T1 to T12, a uniformly increasing model was derived for disc and vertebral body sizes using anatomical literature. We found that the major axis of the ellipse (long axis of an oval) is parallel to the posterior body margin of T12, whereas the minor axis of the ellipse (short axis of the oval) passed through the superior  endplate of T12. The minor axis to major axis ratio was computed to be 0.69.4 Figure 4 shows this optimized elliptical model in a template form that can be used for any height of a patient.
endplate of T12. The minor axis to major axis ratio was computed to be 0.69.4 Figure 4 shows this optimized elliptical model in a template form that can be used for any height of a patient.
In the more recent literature, investigators have begun to develop individual subject optimized geometric sagittal plane curve models for thoracic kyphosis.10-12 There are certain anatomic variables that have been shown to have a moderate influence on sagittal plane curvature. When these anatomic variables are outside of normal tolerances, a change in sagittal curvature can result. This information will be detailed in Part 2 of this series.
Summary
Chiropractic has a long history of identifying and attempting to restore normal alignment to the spine, where abnormal alignment is specifically referred to as the mechanical component of vertebral subluxation. The key is to fully understand when the modelling and alignment data presented herein is useful in differentiating a subluxated thoracic spine from a normal spine and how to modify the data and intervene in specific patient situations. Till next time.
Dr. Deed will be presenting a comprehensive, contemporary review of this topic at the upcoming 33rd CBP Annual Conference on Sept. 23-25th, in Phoenix, AZ.
References
• Harrison DD. Spinal Biomechanics: A Chiropractic Perspective. National Library of Medicine #WE 725 4318C, 1982-97.
• Harrison DE, Cailliet R, Harrison DD, Janik TJ, Holland B. Centroid, Cobb or Harrison Posterior Tangents: Which to Choose for Analysis of Thoracic Kyphosis? Spine 2001; 26(11): E227-E234.
• Harrison DE, Janik TJ, Harrison DD, Cailliet R, Harmon S. Can the thoracic kyphosis be modeled with a simple geometric Shape? The results of circular and elliptical modeling in 80 asymptomatic subjects. J Spinal Disord Tech 2002; 15(3): 213-220.
• Harrison DD, Harrison DE, Janik TJ, Cailliet R, Haas JW. Do alterations in vertebral and disc dimensions affect an elliptical model of the thoracic kyphosis? Spine 2003;463-469.
• Fon GT, Pitt MJ, Thies AC Jr. Thoracic
• kyphosis: range in normal subjects. AJR 1980;134(5):979-83.
• Harrison DE, et al. How Do Anterior/Posterior Translations of the Thoracic Cage Affect the Sagittal Lumbar Spine, Pelvic Tilt, and Thoracic Kyphosis? Eur Spine J 2002;11:287-293.
• Harrison DE, Colloca CJ, Keller TS, Harrison DD, Janik TJ. Anterior thoracic posture increases thoracolumbar disc loading. Eur Spine J 2005; 14:234-242.
• Kiefer A, Shirazi-Adl A, Parnianpour M. Synergy of the human spine in neutral postures. Eur Spine J 1998; 7:471-479.
• Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine 2005;30:2024-2029.
• Berthonnaud E, et al. Analysis of the sagittal balance of the spine and pelvis using shape and orientation parameters. J Spinal Disorders & Techniques 2005;18(1):40-47.
• Vaz G, Roussouly P, Berthonnaud E, Dimnet J. Sagittal morphology and equilibrium of pelvis and spine. Eur Spine J 2002; 11(1):80-87.
• Vialle R, Levassor N, Rillardon L, Templier A, Skalli W, Guigui P. Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surgery 2005;87Am:260-267.