DISCUSSION FROM DR. DAN MURPHY
Oxygen is required to make adenosine 5’-triphosphate (ATP). Chronic hypoxia results in reduction of ATP. The body will respond by increasing anaerobic glycolysis, resulting in increased pyruvate production and increased lactic acid, both of which increase pain perception. The pain of fibromyalgia is caused, in part, by hypoxia (which is, in itself, painful) and the increase of lactic acid from increased anaerobic glycolysis.
Glucose is also required to make ATP. Therefore, the body will also respond by attempting to increase the genesis of glucose. The body can make glucose for the purpose of producing ATP by assembling it from smaller molecules, especially from amino acids. The process of assembling glucose from smaller molecules is termed gluconeogenesis. To make glucose from amino acids, the body has to break down proteins, a process termed proteolysis, and the best source of protein for this purpose is from the muscles. The pain of fibromyalgia is also caused by the proteolysis of muscle tissue that occurs in order for the required gluconeogenesis to increase ATP synthesis in these patients.

KEY POINTS FROM DR. DAN MURPHY:
1. “Fibromyalgia (FM) is a common clinical syndrome of generalized musculoskeletal pain, stiffness and chronic aching, characterized by reproducible tenderness on palpation of specific anatomical sites, called tender points.”
2. Fibromyalgia is primary when not associated with systemic causes, trauma, cancer, thyroid diseases and pathologies of rheumatic or connective tissues.
3. “FM is nine times more common in middle-aged women (between the ages of 30 and 50 years) than in men.”
4. The best proposed etiology for fibromyalgia is chronic hypoxia.
5. These authors propose that fibromyalgia symptoms are predominantly caused by enhanced gluconeogenesis with breakdown of muscle proteins, resulting from a deficiency of oxygen and other substances needed for ATP synthesis.
6. Magnesium and malate have a critical role in ATP production and, therefore, fibromyalgia symptoms may be caused by magnesium and malate deficiency.
7. Fibromyalgia is associated with irritable bowel syndrome, tension headache, primary dysmenorrhea, mitral valve prolapse and chronic fatigue syndrome.
8. Various treatment modalities have been tested in FM patients with poor results, including tryptophan, ibuprofen, and tricyclic drugs.
9. “Elevated catecholamines are observed in urine of FM patients.” [Important: elevate catecholamines (norepinephrine and epinephrine) are the result of increased sustained sympathetic tone. Increased sustained sympathetic tone can be the consequence of reduced mechanical integrity, such as a vertebral subluxation.]
10. Reduced oxygen reduces ATP synthesis. Oxygen is reduced by hypoxia, magnesium deficiency, malate deficiency.
11. Magnesium is reduced by excess aluminum and/or excess calcium.
12. ATP production is controlled by the vitamins thiamine (B1), riboflavin (B2), and pyridoxine (B6) because they are essential for the electron transport system, and all three vitamins require magnesium to become biologically active.
13. During anaerobic glycolysis, from glucose to acetyl-Co A, there are eleven distinct steps; nine of the eleven [82 percent] steps require magnesium.
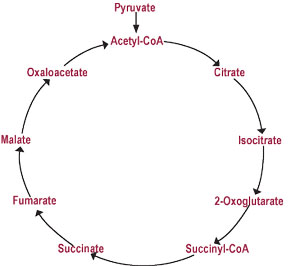
14. The Krebs Cycle (Citric Acid Cycle) has nine steps, and three of them require magnesium.
15. An “adequate oxygen supply enhances ATP yield by 18-19 fold.”
16. Fibromyalgia symptoms improve following aerobic conditioning.
17. Aluminum has a high affinity for phosphate and blocks the absorption and utilization of phosphate for ATP synthesis, causing decreased mitochondrial ATP levels. Adequate levels of magnesium prevent this toxic effect of aluminum.
18. Malic acid is one of the most potent chelators of aluminum and is most effective in decreasing brain aluminum levels.
19. “The most common symptoms associated with FM—myalgia, chronic fatigue syndrome, irritable bowel syndrome, mitral valve prolapse, tension headache and dysmenorrheal—have been reported in patients with magnesium deficiency, and magnesium supplementation improves these symptoms.”
20. Malate deficiency is the cause of the ATP deficiency seen with exhaustive physical activity.
21. “In humans as well as in other animals tested, when there is increased demand for ATP, there is also an increased demand and utilization of malate.”
22. Malate demands are greater in hypothyroid fibromyalgia patients.
23. Fibromyalgia patients supplemented with a daily dose of 300-600 mg magnesium plus 1200-2400 mg of malic acid “all patients reported significant subjective improvement of pain within 48 h of starting.” Additionally, the fibromyalgia tender point scores were reduced by about 60 percent at four weeks and 66 percent at eight weeks.
COMMENTS FROM DR. DAN MURPHY
Each capsule of the malic acid plus magnesium supplement I use in the management of fibromyalgia patients contains 294 mg of malic acid and 59 mg of magnesium. Each capsule also contains a balance of compounds that have also been shown to benefit patients with fibromyalgia: grapeseed extract, betatine HCL, silymarin extract, bromelain, papain, trypsin, lipase, amylase, pancreatin, lecithin (phosphytidal choline), l-leucine, l-valine, glucosamine sulfate, N-acetyl glucosamine, and ornithine alpha keto-glutarate.
Another article [Article 17-07: Treatment of Fibromyalgia Syndrome with Malic Acid: Journal of Rheumatology, May 1995;22(5):953-8] suggests that the minimum dosage should be six tablets per day (two with each meal), which would supply 1,764 mg of malic acid and 354 mg of magnesium. For some patients, the optimal dosage should be nine tablets per day (three with each meal), supplying 2,646 mg of malic acid and 531 mg of magnesium.
Reference
“Management of Fibromyalgia: Rationale for the Use of Magnesium and Malic Acid” by Guy E. Abraham, M.D., and Jorge D. Flechas, M.D., M.P.H. Journal of Nutritional Medicine No. 3, 1992, pp. 49-59.
Dr. Dan Murphy graduated magna cum laude from Western States Chiropractic College in 1978. He received Diplomat status in Chiropractic Orthopedics in 1986. Since 1982, Dr. Murphy has served part-time as undergraduate faculty at Life Chiropractic College West, currently teaching classes to seniors in the management of spinal disorders. He has taught more than 2000 postgraduate continuing education seminars. Dr. Murphy is a contributing author to both editions of the book Motor Vehicle Collision Injuries and to the book Pediatric Chiropractic.