TAC: How do chiropractors generally pick the techniques that they perform?
Roth: Chiropractors and other health professionals are drawn to techniques and theories that will help them move to the next level. As each practitioner evolves in skill and understanding, they naturally reach for higher ground. And, as it has been said, “When the pupil is ready, the teacher appears.”
I have consistently found, too, that it is only through this desire to provide better service, that the door to financial success is opened. It is through the joy of helping others and experiencing the power of the self-healing process, which we support, that we become open to the positive flow assuring personal and monetary success.
TAC: We often hear that one technique does not always work on every patient a doctor sees. What do you think about this statement?
Roth: There are many techniques that work, and the ones that work best are the ones that gently encourage the body’s natural ability to be restored to optimal health and well-being.
I also believe it is a question of attitude. If the practitioner has an approach that makes sense to him or her, then they are capable of helping their patients to align with the potential to allow the healing to take place.
 TAC: How many techniques should a chiropractor know for the best care of their patients?
TAC: How many techniques should a chiropractor know for the best care of their patients?
Roth: It is really not a question of the number of techniques. It is more a question of skill combined with the ability to communicate the larger idea–the goal being to support and encourage the individual toward their potential for healing and wellness. Various techniques may appeal, initially, to different patients; but, once inside the door, it is really their connection to these underlying principles that will make the difference.
TAC: When does a chiropractor know enough about technique that he doesn’t need to learn anymore?
Roth: It is never possible to stop learning. It may be a technique or a philosophy, which helps the practitioner to become clear in his or her goals. This is what will ultimately satisfy the desire to continue growing as a health practitioner and teacher of well-being. This process never ends. When it does, it is time to consider a new career.
George Roth, DC, can be reached at Wellness Systems, Inc., toll-free 1-877-905-7684; Fax: 905-880-0650; e-mail [email protected]; or visit www.matrixrepatterning.com.
Following are alphabetized descriptions of this edition’s Ten Great Techniques, with brief discussions of their evolution, theories and applications.
The Bio Cranial System
 The Bio Cranial System (BCS), probably for the first time, links the spine and cranium as one complete and inseparable unit. This is the conclusion arrived at by United Kingdom based osteopath Robert Boyd, DO, whose teachings are now being taught widely to doctors of chiropractic. Hence, the patient suffering from low back pain, sciatica, headaches, diabetes, dysmenorrhea, chronic fatigue, etc., is, from a Bio Cranial perspective, suffering globally from a total physiological disturbance.
The Bio Cranial System (BCS), probably for the first time, links the spine and cranium as one complete and inseparable unit. This is the conclusion arrived at by United Kingdom based osteopath Robert Boyd, DO, whose teachings are now being taught widely to doctors of chiropractic. Hence, the patient suffering from low back pain, sciatica, headaches, diabetes, dysmenorrhea, chronic fatigue, etc., is, from a Bio Cranial perspective, suffering globally from a total physiological disturbance.
After many years of research, Dr. Boyd concluded that Sutherland’s Primary Respiratory Mechanism was the basis from which all function (physiology) derived. This included not only visceral function but, crucially, also the musculoskeletal system. His conclusions were first announced to the world in 1988 in his first book, An Introduction to Bio Cranial Therapy. He concluded that, while segmental subluxations were certainly present, they were almost always secondary, and compensatory, to the totality of the craniosacral system’s “lesion”.
The anatomical disposition of the cranial bones is flawed with just about everyone as part of the birthing (and pre-birthing) event. The next casualty in the chain is the dural membrane. Since, therefore, the spine is essentially representative of the cranial disposition, Dr. Boyd believed that the need was to change the cranial (and therefore dural) status, and there was no requirement to address the spine at all–even for most extremity problems.
Unlike most, if not all, cranial approaches, The Bio Cranial System takes no more than 2-3 minutes to deliver and is relevant to almost all disorders.
The Bio Cranial Institute is dedicated to the training of both the philosophical and technical aspects of the Bio Cranial System worldwide to qualified healthcare practitioners. For more information, call 1 718-886-6056, or visit www.biocranial.com.
Bio-Kinetics Health System
 1956 Palmer graduate, developer and patent holder of Bio-Kinetics Health Systems and New-Stim Stimulator, Dr. Lawrence E. Newsum, has been a seeker of health his entire career, and subscribes to the philosophy that health is a state of normal function on physical, emotional, chemical and spiritual planes of existence.
1956 Palmer graduate, developer and patent holder of Bio-Kinetics Health Systems and New-Stim Stimulator, Dr. Lawrence E. Newsum, has been a seeker of health his entire career, and subscribes to the philosophy that health is a state of normal function on physical, emotional, chemical and spiritual planes of existence.
The Bio-Kinetics approach accesses the body’s response to cellular memories of past traumas of every type: physical, structural, organ related, mental-emotional, environmental, food toxicities, allergies, and even man-made electromagnetic frequencies. All memories translate into energy frequencies, and have the potential of enhancing or disrupting the ideal function of the whole integrated system of the brain and body.
 Dr. Newsum developed a protocol to locate and normalize, or neutralize, the body response to those memories which, when accessed, are easily demonstrated through the monitoring of changes in muscle response, structural balance, leg and arm length, change in blood pressure, physiological blind spots, bio-electrical skin response and many other tests.
Dr. Newsum developed a protocol to locate and normalize, or neutralize, the body response to those memories which, when accessed, are easily demonstrated through the monitoring of changes in muscle response, structural balance, leg and arm length, change in blood pressure, physiological blind spots, bio-electrical skin response and many other tests.
He discovered that, by introducing a small amount of mechanical stimulation into the richest bed of neuro-receptor sites in the upper cervical region on precise sites and directions, powerful brain activation and normalization of feedback and memory loops was accomplished, normalizing aberrant frequencies. Malfunction on any level indicates aberrant, abnormal frequency of firing of neurons. With the unique stress/correct/stress/correct cycles and New-Stim stimulation, Bio-Kinetics re-educates and re-integrates neuro-receptor pathways, and restores health.
For the past 12 years, Dr Newsum has been teaching chiropractors worldwide how to utilize Bio-Kinetics on their patients, families and even themselves through New-Stim Bio-Kinetics Seminars. For more information, call 310-325-9122 or visit www.biokineticshealth.com.
Body Integration
Body Integration is a diagnostic and treatment method of healthcare procedures which allows the body to reveal the underlying cause of the symptoms exhibited. The body has many complicated functions and an unfathomable data bank. Body Integration helps translate the mystery of the body and lets the body write its own instruction manual. There is no easy answer to any problem. However, Body Integration looks at the blueprint of the body, and with advanced healthcare procedures, allows the body to reveal the underlying cause of the symptoms exhibited.
The main objective is to find the basic underlying cause of the problem by completing a comprehensive, diagnostic workup which includes confidential consultation, a carefully taken case history and a complete examination. Muscles have electrical qualities and rely on a properly working glandular system, nervous system, circulatory system, endocrine system, acupuncture system, and many other systems of the body. Our inability to adapt to the stresses of life can be measured to a great extent by diagnosing the errors in our muscular system. This includes a therapeutic approach to food and nutrition therapy designed especially for each individual’s needs.
Coming in late summer is a 16-volume manual and computer program with total body integration of myomeres, vertebral levels, cranial bones, foot bones, acupuncture points, extremities, organs, tissues, hand bones, nutrients, emotions, lymph nodes, the brain and an instruction manual.
Body Integration was developed by René Thomas (Espy), DC, who has taught many practitioners worldwide how to determine the primary subluxation. For more information, call 1-866-497-8273 or visit www.bodyintegration.com.
CranioSacral Therapy (CST)
CranioSacral Therapy is a gentle method of releasing restrictions in the craniosacral system—the membranes and cerebrospinal fluid that surround and protect the brain and spinal cord, and have a vital impact on central nervous system performance.
CST was developed by osteopathic physician John E. Upledger. From 1975 to 1983, he led a multidisciplinary team of anatomists, physiologists, biophysicists and bioengineers at Michigan State University to test and document the influence of the craniosacral system on the body. That research formed the basis for the modality Dr. Upledger developed and named CranioSacral Therapy.
Essentially, the craniosacral system functions as a semi-closed hydraulic system, bathing the brain and spinal cord in cerebrospinal fluid pumped rhythmically 6-12 cycles per minute. As fluid volume and pressure rises and falls within the craniosacral system, corresponding changes occur in dura mater membrane tensions. These changes induce accommodative movements in the bones that attach to the dura mater compartment.
When the natural mobility of the dura mater or any of its attached bones is impaired, the function of the craniosacral system—and the central nervous system—may be impaired as well. Such restrictions can be detected and corrected using simple methods of palpation. By normalizing the craniosacral system and enhancing the body’s self-corrective mechanisms, CST has proven effective for a wide variety of dysfunctions and conditions addressed in the chiropractic setting.
More than 65,000 healthcare providers have been trained in CranioSacral Therapy. CEU’s are widely available for doctors of chiropractic.
For more information, call 1-800-233-5880 or visit www.upledger.com.
Creed Neural Kinetic Integration Technique
The Creed Neural Kinetic Integration Technique embodies a positional relationship approach that re-orbits the musculo-skeletal structure,establishing a foundational platform for re-alignment of the head over shoulders, shoulders over hips, and hips over ankles to support the patient’s natural stance. These structural changes re-orient the facet plane angles, reduce the gravitational pulls on muscles and associated nerves, allowing for increased ranges of motion. These changes create truer proprioceptive feedback functions to motor muscle response systems, vertebral joint motion, reflexes, and the reduction of sensory nerve stimuli that cause pain. The outcome is a comprehensive reprogramming of the body’s structural architecture that is clearly communicated to the cerebellum via the Alpha I, II, and III neuro-fibers during the adjustment. The patient experiences rapid relief from pain and discomfort, improved function and ranges of motion.
Pre and post applied functional testing allows the doctor and patient to identify the aberrant conditions prior to treatment and acknowledge the positive changes afterwards. Correcting vertebral subluxations, soft tissue and muscle concurrent with full body postural alignment is performed in various positions: standing, sitting, supine, prone or in motion. Conditions of acute and chronic pain syndrome, disc degeneration, osteophytic activity, scoliosis, failed back surgery, general fatigue as well as other degenerative conditions respond well to this comprehensive approach.
Dr Alan Creed presents a nation-wide seminar series, Boost Your Practice: Bridging Techniques, Styles & Technologies, which is approved for Continuing Education Credits. Dr. Creed is a board eligible chiropractic neurologist and has a chiropractic practice on Key Biscayne, Florida. For more information, call 1-305-365-7988 or visit www.dralancreed.com.
Neuro Physio Balancing
Neuro-Physio-Balancing (NPB) is a system that utilizes body reflexes for analysis and treatment. It is a study of body reflexes.
What are reflexes? Most of the actions of digestion, all immune reactions and almost all muscle function are reflexive. All adjustments use body reflexes. All neurological tests are comparing reflexes (blood pressure, heart rate, etc.) You cannot have a change in pain level or muscle tone following an adjustment without a 100% reflexive response. All symptoms are reflexes; all treatments and all emotions are reflexive reactions.
NPB begins by exploring the subluxation; how it influences the brain and nervous system, circulation in the body, organ function and musculoskeletal system. The key is understanding the autonomic nervous system connection. Various types of direct and indirect muscle tests can lead us to the lesions or subluxations. These can identify missed reductions of a subluxation.
There are fast reflexive procedures to strengthen chronic weak muscles. Most of these chronic weak muscles are a consequence of long-term noceciptive inhibition. This noceciptive inhibition can be unnoticed pain due to receptor fatigue or inhibition due to the chronicity. Stabilizing muscles can sustain a disproportional weakness regardless of therapy or exercise. Certain fast simple procedures can reset the muscles, resulting in immediate, impressive strength increase.
NPB encompasses a full spectrum approach: Adjusting (subluxations), reflex stimulation to reduce sympathetic tone and increase parasympathetic tone to promote organ function, improve blood flow and improve function of the nervous system, musculoskeletal system, brain and emotions.
NPB is designed to be performed primarily by hand. No expensive equipment needed.
Neuro-Physio-Balancing was developed by Richard C. Freeze, BS, DC, DACAN, DACNB. www.drfreeze.prodigybiz.com
The NUCCA Technique
Dr. Ralph R. Gregory founded the National Upper Cervical Chiropractic Association (NUCCA), in 1966, as an orthogonally based upper cervical chiropractic technique using acceptable and predictable scientific principles, including measurement, observation and reason. The technique measures and evaluates postural distortions, thermographic differentials and cervical spine misalignment (with pre- and post-X-rays). Precisely aligned X-ray equipment and stringent patient placement protocols produce X-rays to be analyzed in all three planes of motion, yielding a vectored production/reduction pathway to use to correct the Atlas Subluxation Complex.
The Atlas Subluxation Complex (ASC) is the measured angular relationship between the skull and vertebrae of the cervical spine. The body moves away from a vertical axis in the standing position: high and low pelvis in the frontal plane, twisting of the pelvis in the transverse plane, movement of the upper torso into one of the frontal planes. There is a measurable functional leg length inequality in a prone position and bilateral weight imbalance.
The body returns to frontal and transverse plane symmetry in the standing position when the upper cervical spine is corrected through proper adjustment, stabilizing the spine in a normal position, which removes the neurological interference and minimizes the need for repeated adjustments.
NUCCA has developed a sophisticated biomechanical understanding of the upper cervical misalignment, the specific neurology affected, altered centers of motion and centers of gravity of spinal vertebrae and the correction and stability of the ASC.
For more information, visit the NUCCA website at www.nucca.org.
The Pro-Adjuster Technique
The Pro-Adjuster Technique evolved from the Pierce-Stillwagon Technique combined with computer technology to form a system of patient care that is standardizing the industry. The development of this technology was completed by Dr. Maurice A. Pisciottano, following the passing of Dr. Walter V. Pierce, Sr.
Using a c-posture chair, the patient’s spine is examined while positioned in mild flexion. Each vertebra is analyzed by evaluating the echo response of a mild six-pound percussive force that is introduced to each spinal segment. This force is computer controlled to be exactly the same every time.
The piezoelectric sensor in the instrument records the motion characteristics of the motor units. The data is displayed on the monitor so the doctor can evaluate whether the patient needs an adjustment, and which areas are out of tolerance with regard to fixation, mobility, fluid motion and frequency.
The doctor selects the motor units to be adjusted. The computer calculates a corrective frequency of percussion based upon the analysis just performed. The instrument applies a force until the sensor determines that the harmonic balance has been restored in the area in question. The adjustment automatically stops and the patient is ready for post analysis.
The re-analysis process allows the doctor to immediately compare the original composite to the post composite reading. The specialized hardware and software eliminates the subjective variables. The result is an accurate and reliable re-analysis process. The Pro-Adjuster establishes objective analysis in the inter-examiner realm, with consistency averaging above 90%.
The technique is safe for individuals of all ages and causes no stress on the chiropractor’s body.
For more information, call 1-877-942-4284 or visit www.pro-adjuster.us.
The Test & Response System
In 1974, Herman Stoffels, D.C., made a new discovery in chiropractic. He discovered that the body’s natural circulating energy fields interfered with the clarity of all reflex-testing methods. The pioneering chiropractor experimented with a wide variety of positioning and placements of the body and limbs and found that an entirely new dimension in body response could be realized by a few unusual, but simple, modifications in body and extremity positioning.
When the body assumes this position, its usual bioelectrical flow is changed and the body’s normal strength greatly increases, often nearly doubling. This position is the Test & Response basic testing position, which makes muscular testing much clearer for all.
Therefore, when the patient is lying in the T&R position, when the doctor contacts the real or true primary vertebrae and performs the T&R test, there is a dramatic change in the patient’s strength and energy level. With the identity of the true primary segment, there is now a loss of the magnified strength of the T&R position and also of the normal strength of the body during the T&R test, making a distinct demarcation between the strength and weakness from this test.
During T&R seminars, demonstrations are performed on participants with obviously uncorrectable conditions and the clinical results have been remarkable. For instance, some old injury disabilities nearly overcome in minutes, or a doctor’s wife–a diabetic since early childhood–dropped six units off her normal 24 units of insulin.
For more information, call 805-239-9121 or visit www.testandresponse.com.
Trigenics Myoneural Medicine
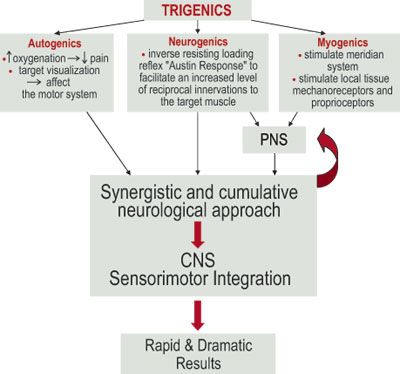
Trigenics is a sensorimotor and energetic restoration system. It incorporates a neurologically-based, multimodal methodology for local or full-body assessment and treatment. Trigenics can be applied as Western manual medicine to correct aberrant sensorimotor function or as Eastern meridian medicine to balance neurosomatic energetics.
Trigenics is used on a very wide variety of patients and conditions. In addition to being used to accelerate rehabilitation and structural correction, Trigenics can be used as an alternative no-force manipulation procedure, and specific Trigenics Sports Augmentation treatments increase athletic power and performance to greater than normal levels.
Trigenics myoneural procedures involve the synergistic, simultaneous application of 3 treatment modalities for a cumulative neurological effect. It’s mode of action works on the basis of integrating neurological convergence projection from both segmental (PNS) and suprasegmental (CNS) pathways. The multimodal stimulation approach utilized in Trigenics is consistent with the principles of neuroplasticity and enhanced corticoneural reorganization of the somatosensory and sensorimotor systems.
Trigenics is often referred to as the “missing link” in neuromusculoskeletal care. In strictly using osseous manipulation to treat the vertebral subluxation complex, not correcting aberrant neurologic input (deafferentation) to the muscular holding elements will lead to the frustrating outcome of chronic, recurring intervertebral dyskinesia. In treating musculoskeletal conditions, non-treatment of aberrant neural innervation and compensatory tone imbalances (short/weak muscles) will lead to the frustrating outcome of incomplete strength rehabilitation and functional restoration. Trigenics provides the solution, by first correcting aberrant proprioceptive neurology (reafferentation). Treatment of aberrant histology (adhesions) and arthrokinetics is then subsequently addressed using soft tissue myofascial techniques and chiropractic procedures.
Trigenics was originated by Canadian-Estonian chiropractor, Dr. Allan Gary Oolo Austin, DC, DAc, CCSP, CCRD, DNM, FIAMA, FTIMM. For more information, call 1-888-514-9355 or visit www.trigenicsinstitute.com. TAC
|
Q:
- Still no info on your favorite Technique, or one you’re curious about? Let us know what we’re missing!
- What’s your best turn-around story after using your favorite technique? Send your story to [email protected] and win a free subscription!
|

 The system operates like a semi-closed hydraulic system based on the rhythmic rise and fall of cerebrospinal fluid volume and pressure in the dura mater. According to research1-8 performed at Michigan State University, the bones directly relating to the dura mater must be in continual, minute motion to accommodate the constant fluid pressure changes within the membrane compartment.
The system operates like a semi-closed hydraulic system based on the rhythmic rise and fall of cerebrospinal fluid volume and pressure in the dura mater. According to research1-8 performed at Michigan State University, the bones directly relating to the dura mater must be in continual, minute motion to accommodate the constant fluid pressure changes within the membrane compartment.  I once saw Tom, who was diagnosed with Bell’s palsy. He woke up one morning to find his face paralyzed. After one office visit, he reported about 50 percent relief. About three weeks of visits later, he considered the problem solved. His emotional outlook was better, too—he had been told he might suffer the effects of Bell’s palsy for months or more.
I once saw Tom, who was diagnosed with Bell’s palsy. He woke up one morning to find his face paralyzed. After one office visit, he reported about 50 percent relief. About three weeks of visits later, he considered the problem solved. His emotional outlook was better, too—he had been told he might suffer the effects of Bell’s palsy for months or more.

 A treatment such as this fits in perfectly with current chiropractic paradigms. The Trigenics Institute of Myoneural Medicine has been teaching Trigenics seminars in Canada and Australia for a number of years. The response from many notable chiropractors that have undertaken its study has been that of high acclaim. The Registered Trigenics Practitioner program and RTP designation were recently introduced to the United States. As such, this article will serve as a brief introduction.Trigenics is an interactive, neurologically based soft tissue assessment and manipulative treatment system that symbiotically combines aspects of both Eastern and Western manual medicines.
A treatment such as this fits in perfectly with current chiropractic paradigms. The Trigenics Institute of Myoneural Medicine has been teaching Trigenics seminars in Canada and Australia for a number of years. The response from many notable chiropractors that have undertaken its study has been that of high acclaim. The Registered Trigenics Practitioner program and RTP designation were recently introduced to the United States. As such, this article will serve as a brief introduction.Trigenics is an interactive, neurologically based soft tissue assessment and manipulative treatment system that symbiotically combines aspects of both Eastern and Western manual medicines. Trigenics is, generally, not hard on the doctor or the patient. It is much easier for the doctor to apply and easier for the patient to receive than regular mechanically based soft tissue techniques. The patient usually does not experience appreciable pain during the treatment, and rarely has any delayed onset of post-treatment soreness. In collectively facilitating the patient’s nervous system to reduce pain signals and inhibit the target muscle, the protocol allows for much easier and even deeper access than would otherwise be achievable.
Trigenics is, generally, not hard on the doctor or the patient. It is much easier for the doctor to apply and easier for the patient to receive than regular mechanically based soft tissue techniques. The patient usually does not experience appreciable pain during the treatment, and rarely has any delayed onset of post-treatment soreness. In collectively facilitating the patient’s nervous system to reduce pain signals and inhibit the target muscle, the protocol allows for much easier and even deeper access than would otherwise be achievable.

 Windows based applications are the appropriate choice today. If you are not familiar with the latest technologies in hardware, networking, and internet connectivity, you should consider hiring a technical person to guide you in making those decisions. Selecting the right hardware and networking system for your software is critical.
Windows based applications are the appropriate choice today. If you are not familiar with the latest technologies in hardware, networking, and internet connectivity, you should consider hiring a technical person to guide you in making those decisions. Selecting the right hardware and networking system for your software is critical.